There is a quiet epidemic unfolding in modern healthcare, and it rarely makes headlines because, on paper, everything looks normal. Millions of men and women wake up exhausted, struggle to lose weight despite disciplined eating, lose hair in the shower, forget simple words mid-sentence, and feel emotionally flattened in ways they cannot explain. They go to their physician, get a blood test, and are told, “Your thyroid is fine,” or worse, “Your medication is working perfectly.” Yet nothing about their lived experience feels fine. This disconnect is not accidental; it is the direct result of an outdated, reductionist approach to thyroid treatment that prioritizes lab values over human physiology. At the center of this problem sits one of the most commonly prescribed medications in the world: T4-only thyroid hormone replacement.
To understand why so many people remain sick on T4-only therapy, one must step back and examine the deeper biology of thyroid function, the historical development of modern thyroid treatment, and the systemic blind spots that have shaped conventional care. The thyroid gland is not merely a hormone factory; it is a conductor orchestrating metabolic rhythm across every cell in the body. When its signals are distorted, the consequences ripple through the brain, heart, digestive system, muscles, and immune network. Yet conventional medicine has reduced this complex system to a single hormone and a single lab marker, creating a model that is convenient for standardization but profoundly inadequate for healing. What follows is a deeper exploration of why this model fails, what it is doing to the body, and how a more complete, physiologically aligned approach—one that includes T3—can restore function.
The Origins of the T4-Only Model: Convenience Over Physiology
The dominance of T4-only therapy did not arise because it is the most effective approach; it emerged because it is the most controllable within a pharmaceutical framework. Decades ago, before synthetic thyroid hormones were widely available, patients were treated with natural desiccated thyroid extracted from animal glands. These formulations contained both T4 and T3, along with other cofactors naturally present in thyroid tissue. Patients often reported significant symptom relief, but dosing variability and lack of standardization made it less appealing to a medical system increasingly focused on precision and uniformity.
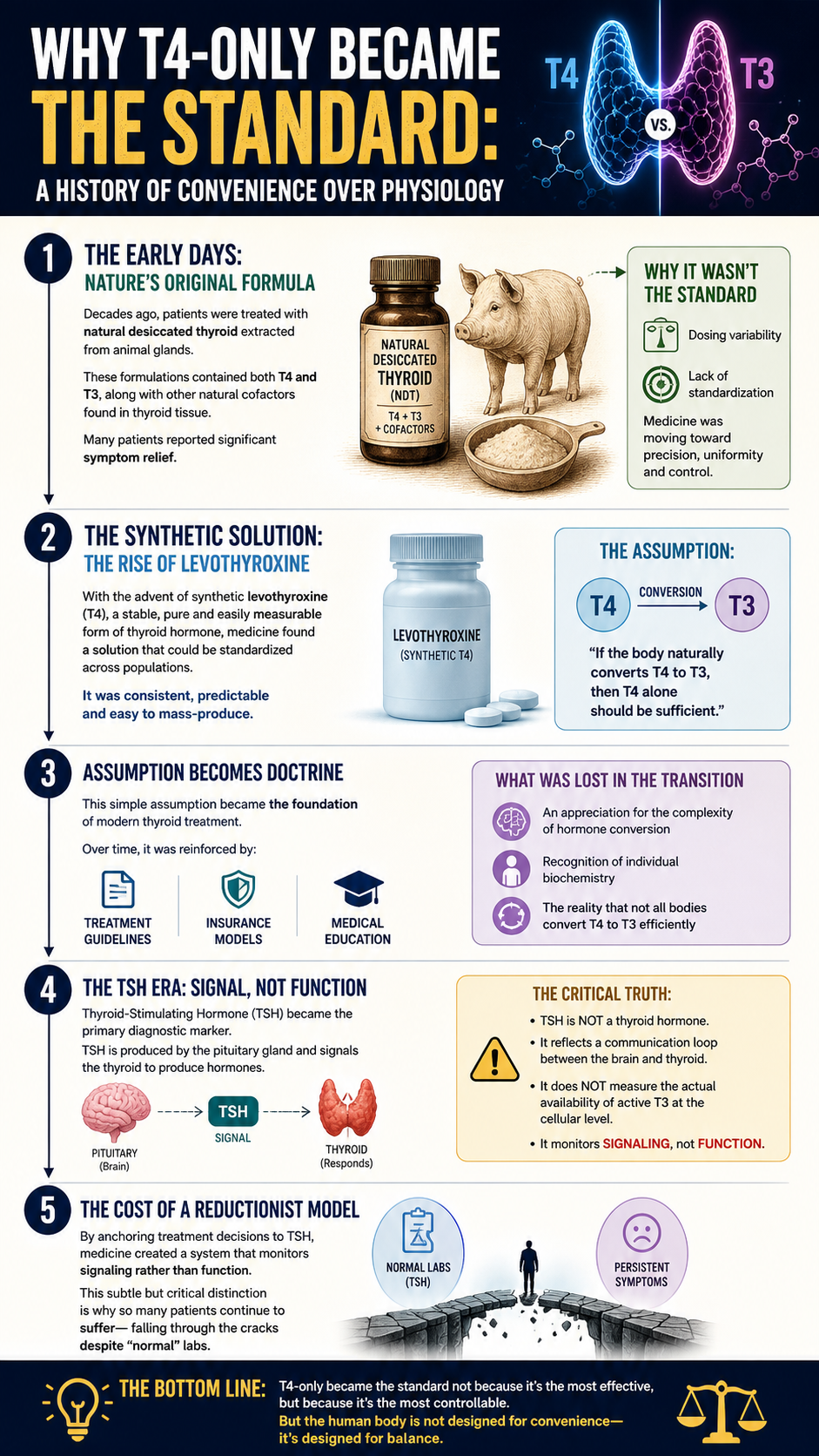
With the advent of synthetic levothyroxine, a stable and easily measurable form of T4, medicine found a solution that could be standardized across populations. The assumption that followed was deceptively simple: if the body naturally produces T4 and converts it into T3, then providing T4 alone should be sufficient. This assumption became doctrine, and over time, it was reinforced by treatment guidelines, insurance models, and medical education. What was lost in this transition was an appreciation for the complexity of conversion, the individuality of human biochemistry, and the reality that not all bodies perform this conversion efficiently.
The reliance on T4-only therapy was further cemented by the widespread adoption of thyroid-stimulating hormone (TSH) as the primary diagnostic marker. TSH is produced by the pituitary gland and signals the thyroid to produce hormones, but it is not itself a thyroid hormone. It reflects a communication loop between the brain and the thyroid, not the actual availability of active hormone at the cellular level. By anchoring treatment decisions to TSH, medicine created a system that monitors signaling rather than function, a subtle but critical distinction that explains why so many patients fall through the cracks.
The Real Physiology: T4 Is Storage, T3 Is Life
At the core of thyroid biology lies a fundamental truth that is often glossed over in clinical practice: T4 is not the hormone that powers your metabolism. T4 is a precursor, a storage form that circulates in the bloodstream waiting to be converted into T3, the active hormone that binds to receptors in your cells. T3 is what enters the nucleus of your cells and influences gene expression, mitochondrial activity, and energy production. It is the difference between potential and action, between stored fuel and combustion.
The conversion of T4 into T3 is not a passive process; it is an active, enzyme-driven transformation that depends on a network of systems functioning optimally. The liver plays a central role in this conversion, using deiodinase enzymes to remove an iodine molecule from T4, transforming it into T3. The gut contributes significantly as well, with the microbiome influencing hormone metabolism and recycling. Nutrient availability, particularly selenium, zinc, and iron, is essential for the enzymes that facilitate this process. Stress hormones, inflammatory cytokines, and environmental toxins can all interfere with conversion, shifting the balance away from T3 and toward an inactive form known as reverse T3.
When this system works as designed, the body maintains a dynamic equilibrium, adjusting T3 levels based on energy demands, stress, and environmental conditions. When it does not, the consequences are profound. Cells become under-stimulated, metabolic processes slow, and the body enters a state of functional hypothyroidism even if circulating T4 levels appear adequate. This is the hidden reality for many patients on T4-only therapy: they have enough storage hormone, but not enough active hormone where it counts.
The Hidden Saboteur: Reverse T3 and Metabolic Shutdown
One of the most overlooked aspects of thyroid physiology is the production of reverse T3 (rT3), an inactive isomer of T3 that acts as a metabolic brake. Under conditions of stress, illness, caloric restriction, or toxin exposure, the body may convert T4 into reverse T3 instead of active T3. This is an adaptive response designed to conserve energy during times of perceived threat, but when it becomes chronic, it creates a state of metabolic suppression that is difficult to escape.
Reverse T3 competes with T3 for receptor binding sites, effectively blocking the action of the active hormone. This means that even if some T3 is present, its ability to exert its effects is diminished. Patients with elevated reverse T3 often experience profound fatigue, cold intolerance, weight gain, and cognitive sluggishness. They may be told their labs are normal because TSH and T4 fall within reference ranges, but at the cellular level, their metabolism is throttled.
T4-only therapy can inadvertently exacerbate this problem by providing more substrate for reverse T3 production. In a body already under stress or burdened by inflammation, additional T4 does not necessarily translate into more T3; it may simply increase the pool of hormone that can be diverted into the inactive pathway. This is one of the key reasons why patients can feel worse, not better, as their T4 dose is increased, a paradox that is rarely acknowledged in conventional care.
What This Is Doing to the Body: The Slow Burn of Cellular Hypothyroidism
When cells are deprived of adequate T3, the effects are not isolated to one system; they are systemic, cumulative, and often misunderstood. The mitochondria, which serve as the energy factories of the cell, rely on T3 to regulate oxidative phosphorylation and ATP production. Without sufficient T3, energy output declines, leading to the pervasive fatigue that characterizes hypothyroidism. This is not the kind of tiredness that resolves with rest; it is a deep, cellular exhaustion that persists regardless of sleep.
The brain is particularly sensitive to thyroid hormone levels, and inadequate T3 can manifest as depression, anxiety, memory impairment, and slowed processing speed. Neurotransmitter synthesis is influenced by thyroid function, and imbalances can disrupt mood regulation in ways that are often misattributed to primary psychiatric conditions. Patients may be prescribed antidepressants or anti-anxiety medications without addressing the underlying hormonal deficiency, compounding the problem rather than resolving it.
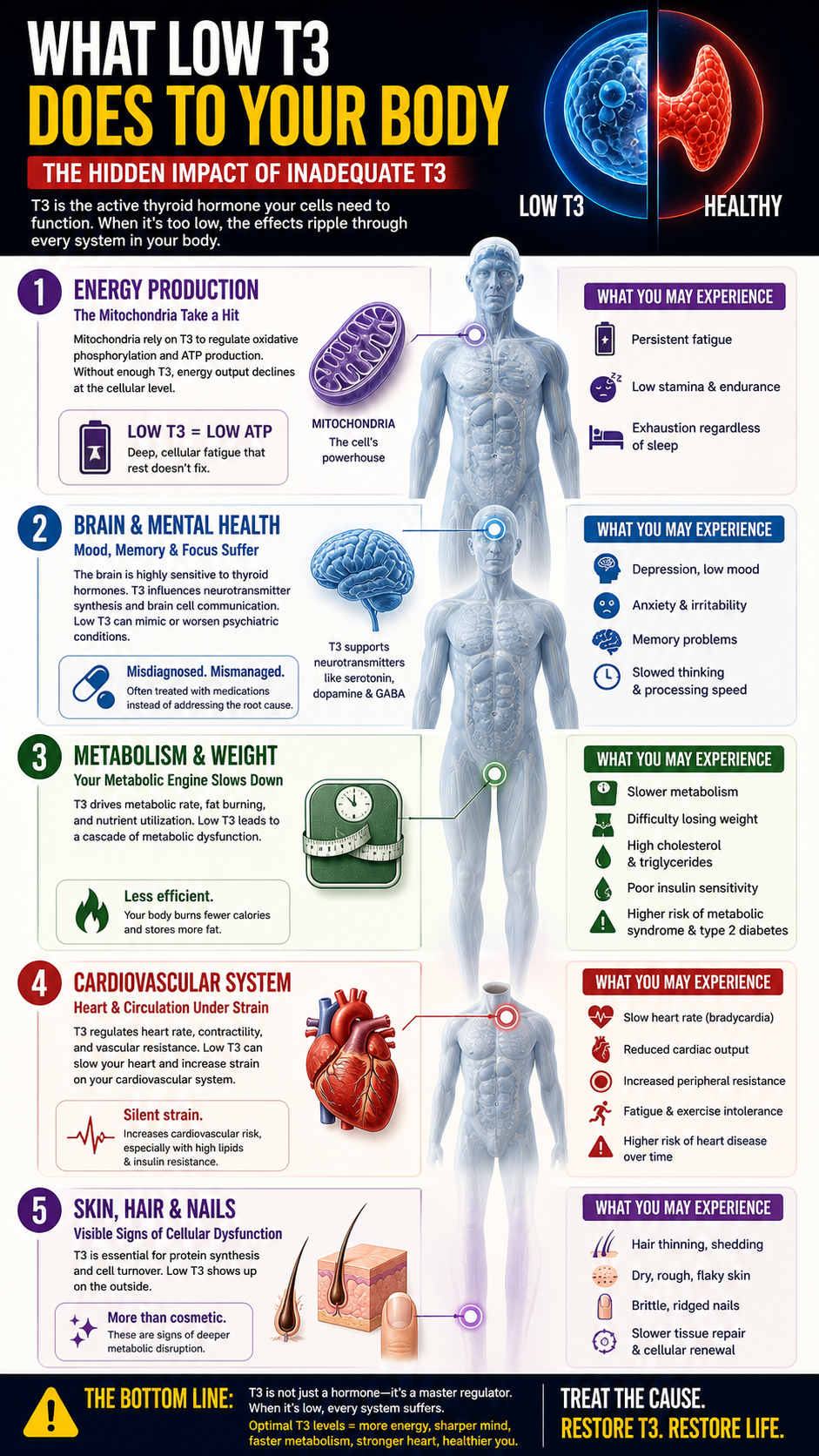
Metabolism, governed in large part by thyroid hormones, slows significantly in the absence of adequate T3. Basal metabolic rate decreases, making weight loss difficult even with caloric restriction. Lipid metabolism is impaired, leading to elevated cholesterol and triglyceride levels. Insulin sensitivity may decline, increasing the risk of metabolic syndrome and type 2 diabetes. The body, in essence, becomes less efficient at utilizing and processing energy, creating a cascade of metabolic dysfunction.
The cardiovascular system is not spared, as T3 influences heart rate, contractility, and vascular resistance. Low T3 levels can lead to bradycardia, reduced cardiac output, and increased peripheral resistance, contributing to fatigue and exercise intolerance. Over time, these changes can increase the risk of cardiovascular disease, particularly when combined with dyslipidemia and insulin resistance.
The skin, hair, and nails often provide visible clues to thyroid dysfunction, as reduced T3 levels impair protein synthesis and tissue turnover. Hair becomes brittle and thin, skin becomes dry and rough, and nails may become weak and ridged. These changes are not merely cosmetic; they reflect a deeper disruption in cellular renewal and metabolic activity.
The Functional Medicine Perspective: Restoring the Full Symphony
Where conventional medicine often reduces thyroid treatment to a single note, functional medicine seeks to restore the entire symphony. This approach recognizes that thyroid health is not determined solely by hormone production, but by conversion, transport, receptor sensitivity, and cellular response. It asks not just whether hormones are present in the სისხod, but whether they are reaching the cells, entering them, and activating the processes they are meant to regulate.
From this perspective, the inclusion of T3 in treatment is not an alternative or fringe approach; it is a logical extension of physiological understanding. If T3 is the active hormone, and if conversion is impaired, then providing T3 directly can bypass the bottleneck and restore function. This can be achieved through combination therapy, using both T4 and T3, or through natural desiccated thyroid, which contains a spectrum of thyroid hormones in ratios more closely aligned with human physiology.
Functional medicine also emphasizes the importance of identifying and addressing the root causes of impaired conversion. This includes evaluating liver function, gut health, nutrient status, stress levels, and toxic burden. It involves looking beyond the thyroid gland itself and recognizing the interconnected nature of the body’s systems. In doing so, it shifts the focus from symptom management to true restoration of health.
T3 Inclusion Protocols: Reintroducing the Active Hormone
T3 inclusion protocols are designed to provide the body with the active hormone it needs while supporting the systems involved in conversion and utilization. These protocols are highly individualized, taking into account the patient’s symptoms, lab values, and overall health status. One common approach is combination therapy, where a small dose of T3 is added to a base of T4, allowing for a more balanced hormonal profile that mimics natural physiology.
Natural desiccated thyroid offers another option, providing both T4 and T3 along with other thyroid components in a single formulation. Many patients report improved symptom control with this approach, as it delivers hormones in a form that the body recognizes and utilizes more readily. In certain cases, particularly where reverse T3 is elevated, a short-term T3-only protocol may be employed to reset receptor sensitivity and reduce the inhibitory effects of reverse T3.
The key to successful T3 inclusion is careful titration and monitoring, as T3 is more potent and has a shorter half-life than T4. Dosing must be adjusted based on both lab values and clinical response, with an emphasis on achieving symptom resolution without inducing hyperthyroid effects. This requires a nuanced understanding of thyroid physiology and a willingness to move beyond rigid protocols in favor of individualized care.
Actionable Steps at Home: Reclaiming Control of Your Thyroid Health
While medication adjustments are an important part of addressing thyroid dysfunction, there are numerous steps that can be taken at home to support conversion, reduce interference, and enhance overall thyroid health. These actions are not substitutes for medical care, but they are powerful complements that can significantly influence outcomes.
Supporting liver function is a foundational step, as the liver is the primary site of T4 to T3 conversion. This involves reducing the intake of alcohol and processed foods, increasing the consumption of nutrient-dense whole foods, and incorporating compounds that support detoxification pathways, such as cruciferous vegetables and bitter greens. Hydration is essential, as it facilitates the elimination of metabolic byproducts and supports overall cellular function.
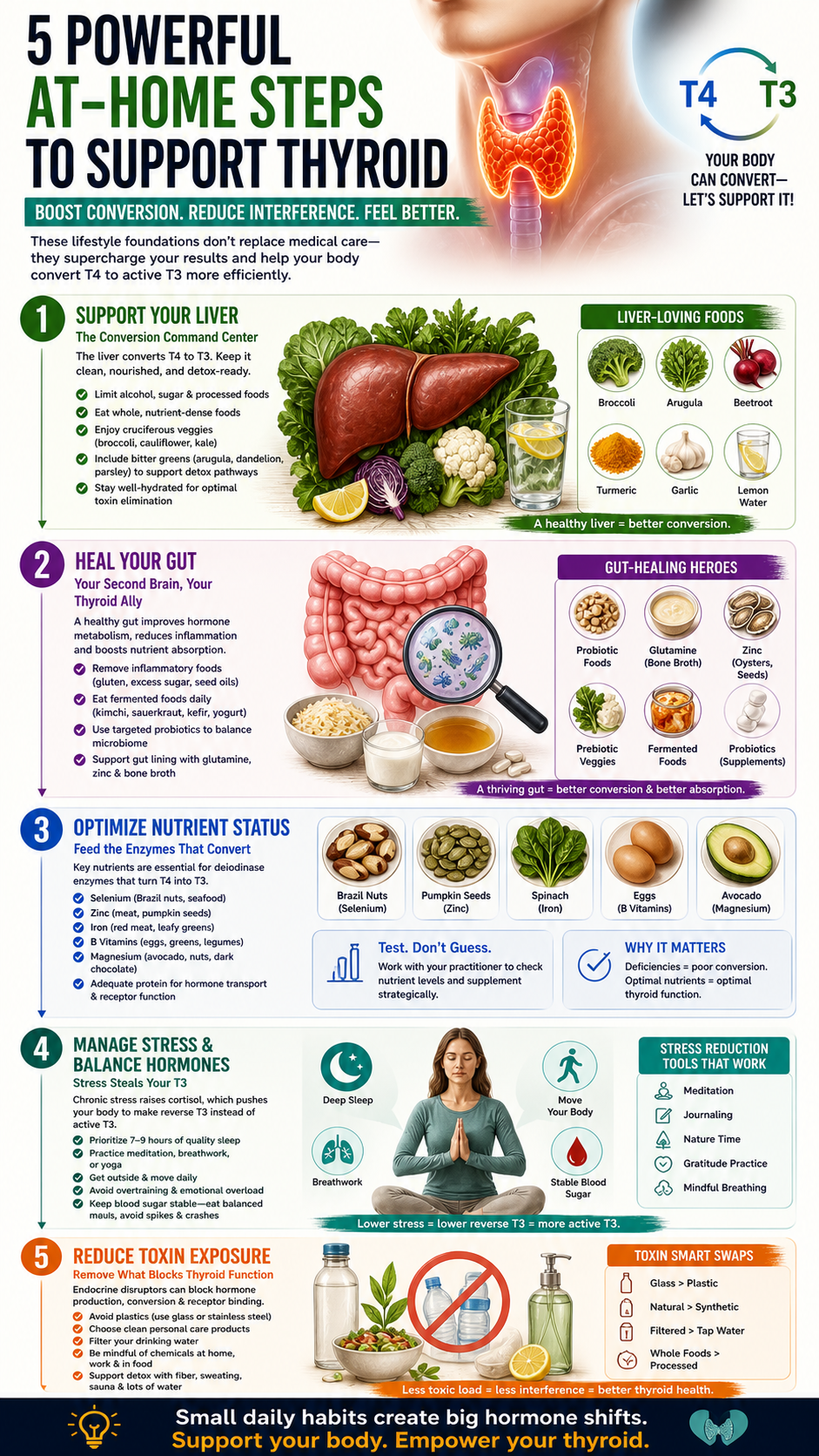
Gut health plays a critical role in thyroid hormone metabolism, and addressing issues such as dysbiosis, inflammation, and increased intestinal permeability can improve conversion efficiency. This may involve eliminating inflammatory foods, incorporating fermented foods or targeted probiotics, and using nutrients that support gut lining integrity, such as glutamine and zinc. A healthy gut environment enhances not only hormone conversion but also nutrient absorption, creating a positive feedback loop.
Optimizing nutrient status is another key component, as deficiencies in selenium, zinc, iron, and B vitamins can impair the enzymes responsible for conversion. This can be addressed through a combination of dietary choices and targeted supplementation, guided by testing where possible. Protein intake should be adequate, as amino acids are necessary for hormone transport and receptor function.
Managing stress is perhaps one of the most challenging yet impactful interventions, as chronic stress shifts the body toward reverse T3 production and disrupts hormonal balance. Prioritizing sleep, engaging in stress-reduction practices such as meditation or breathwork, and avoiding excessive physical or emotional strain can help recalibrate the body’s stress response. Blood sugar stability is also important, as fluctuations can exacerbate stress hormone release and further impair conversion.
Reducing exposure to environmental toxins is an often overlooked but critical step, as endocrine disruptors can interfere with thyroid hormone production, conversion, and receptor binding. This includes minimizing the use of plastic containers, choosing clean personal care products, filtering drinking water, and being mindful of chemical exposures in the home and workplace. Supporting the body’s natural detoxification processes can enhance resilience and improve overall hormonal balance.
The Path Forward: From Suppression to Restoration
The story of T4-only thyroid treatment is not one of malicious intent, but of incomplete understanding and systemic inertia. It is a model that has persisted because it is simple, scalable, and supported by decades of institutional momentum. Yet simplicity is not always synonymous with effectiveness, particularly when dealing with the intricate systems of the human body.
For those who continue to suffer despite “normal” labs and standard treatment, the path forward lies in questioning assumptions, seeking deeper understanding, and embracing a more comprehensive approach. This includes recognizing the central role of T3 in metabolic health, addressing the factors that impair its production and utilization, and being open to treatment strategies that reflect the full complexity of thyroid physiology.
Healing is not achieved by forcing the body into a narrow range of lab values, but by restoring the conditions under which it can function optimally. This requires a shift in perspective, from treating numbers to treating people, from suppressing symptoms to resolving root causes. It is a journey that demands curiosity, persistence, and a willingness to look beyond conventional boundaries.
For many, that journey begins with a simple but transformative realization: the problem is not that their body is broken, but that their treatment has been incomplete. By addressing that gap, by reintroducing the active hormone and supporting the systems that sustain it, it is possible to move from a state of chronic dysfunction to one of renewed vitality.