Osteoporosis Isn’t a Calcium Deficiency—It’s a Collagen and Hormone Problem
For decades, osteoporosis has been marketed to the public as a simple math equation: lose calcium, replace calcium. The story is tidy, memorable, and incomplete. Bones are not inert chalk sticks that merely “run low” on mineral. Living bone is a dynamic organ system—vascularized, innervated, hormonally regulated, and constantly remodeled in response to mechanical load, immune signals, nutrient availability, and endocrine status.
If we zoom in to what a bone actually is, the “calcium deficiency” story starts to look like a misdiagnosis of the problem. Bone strength depends on both mineral and matrix. The mineral (largely hydroxyapatite) confers compressive strength, while the organic matrix—mostly type I collagen—confers tensile strength, ductility, and resistance to crack propagation. In plain terms: mineral makes bone hard, collagen makes bone tough. When collagen quality is compromised, a bone can test “dense enough” and still fracture. When hormones are dysregulated, the remodeling process can be pushed toward breakdown even if calcium intake is high.
This is why a calcium-first approach so often disappoints in real-world outcomes. Calcium matters, but it is not the starring actor. It is a supporting role in a much larger play: collagen integrity and endocrine orchestration.
Bone Is a Composite Material, Not a Rock
Bone is best understood as a composite—an engineered pairing of mineral crystals embedded in an organic scaffold. The organic fraction of bone matrix is dominated by type I collagen, often cited as roughly 90% of the organic matrix. (PMC) This collagen network is not decorative. It is the internal architecture that gives bone resilience, helping it bend microscopically under force rather than snapping like porcelain. Reviews of bone matrix biology emphasize that collagen’s dense, cross-linked structure is central to fracture toughness and crack resistance. (Physiology Journals)
If collagen is poorly formed, inadequately cross-linked, glycated by chronic hyperglycemia, or degraded by excessive catabolic signaling, you can mineralize a structurally inferior scaffold and still end up with brittle bone. That brittleness can show up clinically as fractures that seem “out of proportion” to bone density readings, which is one reason BMD is useful but not sufficient. Bone quality—microarchitecture, turnover rate, collagen cross-link profile, and mineral crystal characteristics—matters profoundly.
The collagen story also reframes why certain nutrients (vitamin C, adequate protein, trace minerals involved in collagen metabolism) and certain exposures (smoking, chronic inflammation, glucocorticoids) have outsized effects on fracture risk that cannot be explained by calcium alone.
Why “Just Take Calcium” Became the Default Story
The calcium narrative became dominant because it contains partial truth. Calcium is required for mineralization, and severe deficiency can compromise bone health. The problem is what happens when we treat “required” as “sufficient,” and then equate bone health with a single number on a label.
When researchers have tested calcium supplementation against hard outcomes, the results have been mixed and often underwhelming in community-dwelling adults. A recent review focusing on calcium supplementation discusses evidence that supplements do not meaningfully reduce fracture risk in many contexts, while still being commonly prescribed. (PMC) In parallel, meta-analytic work continues to debate benefits and risks depending on baseline deficiency status, population characteristics, and whether vitamin D is included. (ClinicalTrials.gov)
Even the safety narrative is more nuanced than many headlines suggest. A 2023 meta-analysis of randomized trials reported no significant association between calcium supplements and major cardiovascular outcomes, while acknowledging uncertainty and the need to consider individual context. (PMC) Meanwhile, other contemporary reviews still caution against excessive supplementation and emphasize balancing benefits and risks. (SAGE Journals) The take-home message is not “calcium is dangerous.” The message is that calcium is not a magic bullet, and oversimplification invites disappointment and side effects without guaranteeing fracture protection.
Bone does not fracture because calcium intake is imperfect. Bone fractures when the system that maintains bone integrity—matrix formation, mineral deposition, turnover regulation, and mechanical adaptation—breaks down.
Collagen: The Missing Foundation in the Osteoporosis Conversation
Collagen is not optional infrastructure
Type I collagen provides the scaffold upon which mineral is deposited, and it is repeatedly described as the dominant organic component of bone matrix in foundational reviews of bone biology. (PMC) Collagen cross-linking patterns, influenced by enzymatic processes and metabolic stressors, are tied to bone mechanical properties. Classic work examining collagen cross-links in bone highlights how matrix chemistry influences strength beyond mineral content. (Wiley Online Library)
This matters because osteoporosis is commonly framed as “porous bone,” but porosity is only one part of fragility. A bone can be porous and tough, or dense and brittle. The difference often lies in matrix quality, turnover dynamics, and microdamage repair.
Clinical evidence that collagen peptides can influence BMD and markers
Collagen supplementation has moved from fringe to testable. A randomized controlled trial in postmenopausal women with age-related BMD reduction reported that specific collagen peptides improved BMD and shifted bone markers toward formation. (PubMed) A later paper focusing on collagen peptides in osteopenia discusses mechanistic plausibility and summarizes human evidence while acknowledging the need for more independent replication. (PMC)
More recently, reviews continue to evaluate collagen peptide supplementation for bone outcomes, reflecting that the field is evolving rather than settled. (Frontiers) The honest interpretation is not that collagen peptides “cure” osteoporosis. It is that collagen support is biologically coherent with bone physiology, and early clinical signals suggest it may be useful as part of a broader strategy—especially when paired with resistance training, adequate protein, and endocrine optimization.
Vitamin C: Collagen Chemistry Disguised as a “Simple Vitamin”
Vitamin C is necessary for collagen synthesis and maturation. When vitamin C is inadequate, collagen formation suffers—an old truth that remains clinically relevant in modern subclinical insufficiency. Observational work from the Framingham Osteoporosis Study investigated vitamin C intake in relation to fracture outcomes. (PMC) A systematic review and meta-analysis of observational studies found that higher dietary vitamin C intake was associated with higher BMD and lower risk of hip fracture and osteoporosis. (Cambridge University Press & Assessment)
Vitamin C’s role is not limited to collagen hydroxylation. Contemporary reviews discuss vitamin C as a regulator of osteogenesis with emerging epigenetic angles, suggesting its influence may extend beyond the classic deficiency model. (OUP Academic)
Again, the point is not to crown vitamin C as a single solution. The point is that collagen biology is inseparable from bone biology, and vitamin C is a quiet gatekeeper of that biology.
Protein: Bone Is Not Built From Minerals Alone
Bone is a protein-based matrix mineralized over time. That simple fact makes chronically low protein intake a predictable risk factor for bone loss and fracture, especially in older adults where sarcopenia and falls compound the danger.
A 2021 study examining dietary protein intake in older adults reported that higher protein intake was associated with higher BMD at multiple sites and lower vertebral fracture risk. (PMC) Large prospective dietary research continues to find inverse associations between protein intake and hip fracture risk, though effect sizes vary and context matters. (Clinical Nutrition Journal)
Protein is also how you build and maintain muscle. Muscle is how you generate the mechanical loading that tells bone to adapt. And muscle is how you prevent falls. Any bone strategy that neglects protein and strength training is fighting with one hand tied behind its back.
Hormones: The Master Regulators of Bone Remodeling
If collagen is the scaffold, hormones are the construction crew and the building inspector. They decide whether you build, maintain, or demolish.
Estrogen: bone’s anti-resorptive signal
Estrogen deficiency is one of the clearest drivers of accelerated bone resorption, which is why postmenopausal bone loss is so common and so rapid early after menopause. The Women’s Health Initiative hormone therapy trials demonstrated increased BMD and reduced fractures with estrogen plus progestin, including reduced hip fracture risk, even though overall risk–benefit considerations are complex and not universally favorable. (PubMed)
If you want a real-world “experiment” demonstrating estrogen’s bone role, look at aromatase inhibitors. These therapies lower estrogen profoundly and are consistently associated with bone loss and increased fracture risk, leading to guideline-driven monitoring and prophylaxis in higher-risk patients. (PMC) This is endocrine physiology written in clinical outcomes: when estrogen signaling drops, resorption rises.
Thyroid signaling: too much turnover becomes net loss
Thyroid hormone excess accelerates bone turnover. When turnover is too fast, bone can become structurally weaker because remodeling units do not fully restore microarchitecture before the next cycle begins. Large studies and meta-analyses have examined associations between subclinical thyroid dysfunction and fracture risk, with evidence supporting increased risk in certain subgroups, particularly with subclinical hyperthyroidism. (JAMA Network)
This matters clinically because thyroid over-replacement is common in practice, and “within range” labs do not always mean “bone-safe” physiology for a specific patient. Bone is a downstream tissue that pays the price for chronic endocrine drift.
Glucocorticoids: catabolic hormones with direct skeletal toxicity
Glucocorticoid-induced osteoporosis is one of the strongest examples of osteoporosis as a hormone problem. Modern reviews describe how glucocorticoids suppress osteoblast and osteocyte function, promote apoptosis in bone-forming cells, and alter osteoclast activity, resulting in rapid fragility. (The Lancet) Even when calcium and vitamin D are given, the hormonal signal still pushes the remodeling balance toward net loss and impaired quality.
If a patient is on chronic steroids, addressing calcium alone is like repainting a house while termites are active in the beams. It looks like action, but it misses the mechanism.

Mechanical Loading: The Signal That Tells Bone to Improve
Bones respond to strain. Without meaningful mechanical loading, the body has little reason to maintain dense, tough bone because it is metabolically expensive tissue.
One of the most cited examples is the LIFTMOR randomized controlled trial, where high-intensity resistance and impact training improved indices related to bone strength and functional performance in postmenopausal women with low bone mass under supervised conditions. (PubMed) This study matters because it challenges the reflexive fear that intensity is always unsafe for osteoporosis. The more accurate stance is that intensity must be dosed, coached, and individualized, but it is often necessary to generate an osteogenic stimulus.
Mechanical loading also strengthens muscle and improves balance, reducing fall risk. Since many fractures are fall-related events rather than spontaneous bone “collapse,” building strength and stability is not optional—it is central.
Vitamin K2 and “Bone Quality” Conversations That Calcium Can’t Touch
Vitamin K-dependent proteins such as osteocalcin are involved in bone mineralization regulation. That mechanistic plausibility has driven trials of vitamin K2 (MK-7), with mixed findings. Some studies report improved vitamin K status and favorable changes in markers and bone strength indices, while other longer trials did not show significant differences in BMD when both groups received calcium and vitamin D. (PubMed)
Systematic reviews and meta-analyses reflect this heterogeneity and suggest that effects may depend on baseline status, dose, population, and endpoints chosen (BMD versus microarchitecture versus fracture outcomes). (Frontiers) The practical conclusion is that vitamin K2 is biologically relevant to bone, but it is not a universal substitute for strength training, protein sufficiency, or endocrine correction.
A More Accurate Framework: Osteoporosis as a Systems Problem
If we stop asking, “How do I get more calcium into bone?” and start asking, “Why is bone remodeling skewed toward breakdown, and why is matrix quality impaired?” the clinical map becomes clearer.
A systems-based osteoporosis model pays attention to:
- Matrix integrity: collagen synthesis, cross-linking, glycation burden, oxidative stress, and nutrient cofactors. (Physiology Journals)
- Endocrine signals: estrogen/androgen balance, thyroid signaling, cortisol/glucocorticoid exposure, insulin/IGF-1 axis, and vitamin D/PTH dynamics. (PubMed)
- Mechanical adaptation: progressive loading, resistance training, impact where appropriate, and fall-prevention fitness. (PubMed)
- Inflammation and medications: chronic inflammatory states, smoking, alcohol excess, proton pump inhibitor considerations, steroids, aromatase inhibitors, and other bone-active drugs. (PubMed)
- Nutrition beyond calcium: protein adequacy, vitamin C sufficiency, magnesium status, and overall dietary quality that supports muscle and metabolic health. (PMC)
This framework does not deny mineral. It places mineral back into its proper context: a necessary ingredient that fails when the recipe is broken.
Practical, Evidence-Informed Priorities
This section is educational and not personal medical advice. Osteoporosis management should be individualized, especially for people with prior fragility fractures, very low T-scores, chronic steroid use, cancer therapies, kidney disease, or complex endocrine conditions.
1) Build the scaffold and the muscle that protects it
A bone plan that does not include progressive resistance training is incomplete. The LIFTMOR trial supports that well-supervised high-intensity resistance and impact training can be both effective and safe in appropriate candidates. (PubMed) Start with coaching and gradual progression, particularly if there is vertebral fracture history or high fall risk.
2) Treat protein as structural, not optional
Aim for sufficient daily protein, especially in older adults. Observational and clinical literature consistently links higher protein intake with better bone outcomes and lower fracture risk in many populations. (PMC) Pair protein intake with strength training so amino acids are “spent” on functional tissue rather than simply oxidized.
3) Ensure vitamin C sufficiency as a collagen lever
Higher vitamin C intake is associated with better BMD and lower fracture risk in meta-analytic observational work. (Cambridge University Press & Assessment) In practice, this often means consistently eating vitamin C-rich foods rather than sporadic supplementation, unless a clinician identifies a specific need.
4) Reassess endocrine drivers instead of treating the skeleton in isolation
Postmenopausal estrogen decline, thyroid hormone excess, and glucocorticoid exposure are all strongly tied to fracture risk through remodeling effects. (PubMed) For patients on aromatase inhibitors, bone surveillance and proactive countermeasures are standard because estrogen depletion predictably harms bone. (PubMed)
This is where functional thinking shines: identify the upstream signal and change it, rather than obsessing over downstream mineral.
5) Use calcium strategically, not reflexively
Dietary calcium adequacy matters, but supplementation decisions should consider diet, labs, kidney stone risk, medications, baseline vitamin D status, and total risk profile. Reviews continue to debate fracture efficacy in broad populations and discuss safety considerations. (PMC) If calcium is used, it should be part of a matrix-and-hormone strategy, not a stand-alone solution.
6) Consider magnesium and other cofactors that support bone metabolism
Magnesium intake has been associated with bone health measures, and a systematic review and meta-analysis in older adults evaluated magnesium intake in relation to BMD and fracture outcomes. (PubMed) This does not mean “megadose magnesium fixes osteoporosis.” It means bone metabolism is mineral-cofactor dependent in ways far broader than calcium.
7) Collagen peptides may be a reasonable adjunct for some people
Human RCT evidence suggests potential benefits of specific collagen peptides on BMD and bone turnover markers in postmenopausal women, with ongoing research continuing to refine who benefits most and under what conditions. (PubMed) Collagen is best viewed as scaffold support, not a replacement for loading and endocrine correction.

Why This Reframe Matters Clinically
When osteoporosis is treated as “calcium deficiency,” patients are often given a supplement and a vague suggestion to “do weight-bearing exercise,” then told to wait for the next scan. That approach can miss the real drivers: inadequate muscle and loading, protein insufficiency, silent endocrine imbalances, chronic inflammation, medication effects, and collagen degradation.
When osteoporosis is treated as a collagen-and-hormone problem, the conversation shifts from passive supplementation to active restoration. You evaluate remodeling signals. You build strength. You support matrix biology. You pay attention to the body’s instructions to bone—because that is what hormones and mechanics are: instructions.
The goal becomes not merely denser bones, but tougher bones, steadier bodies, fewer falls, and fewer fractures. That is a higher standard than a calcium pill can deliver, and it matches what bone physiology has been saying all along.
Absolutely — here’s a clean, in-order resource list exactly as they appeared in the article, formatted so you can use it for citations, footnotes, or a reference section.
Why “Bone Building Medications” Can Improve Your DEXA While Weakening Bone Quality
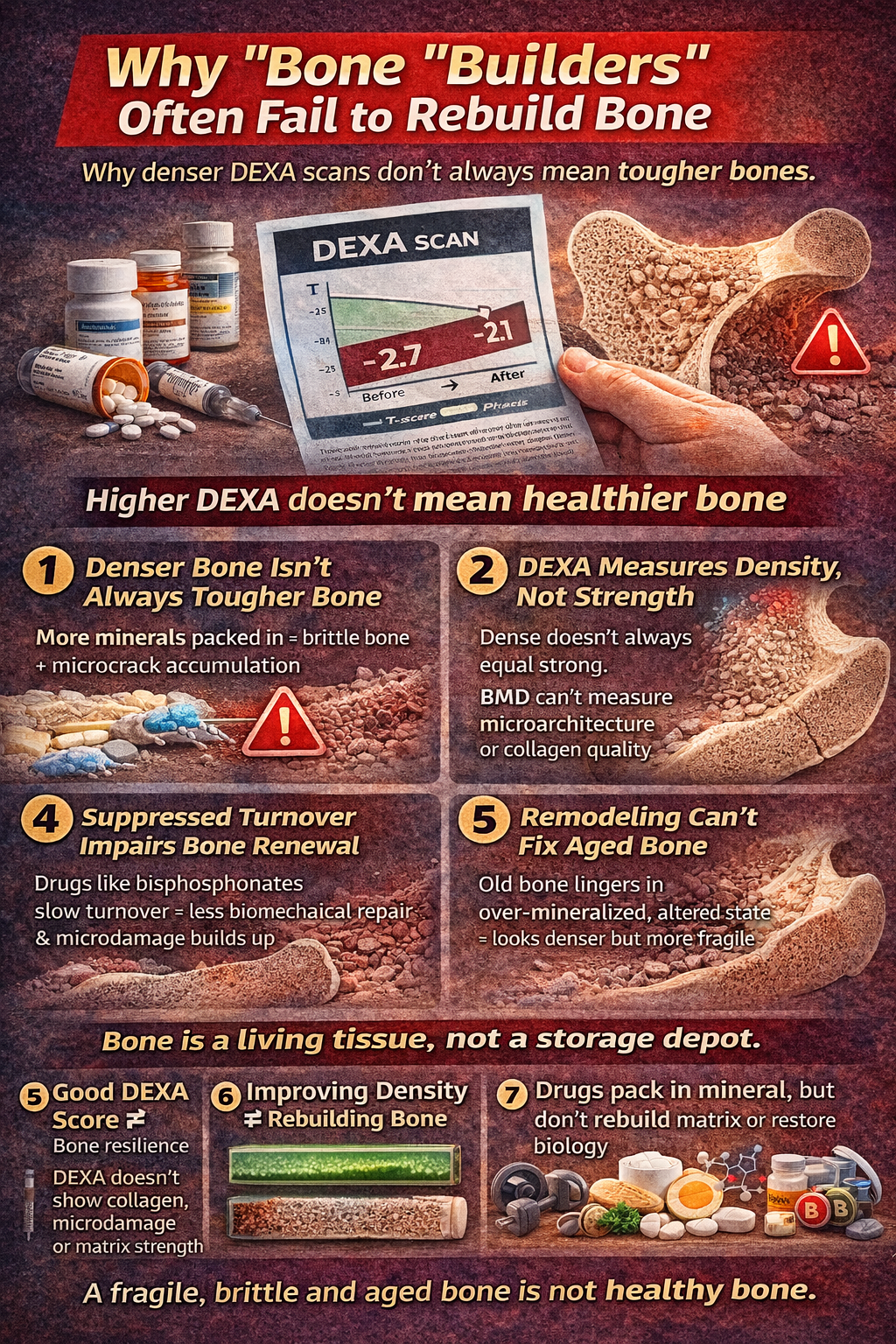
A rising bone density number on a DEXA scan is often treated as proof that bone has been rebuilt. It feels reassuring. The problem is that DEXA measures mineral density, not structural integrity, collagen quality, microarchitecture, or fracture toughness. Bone strength is not identical to bone density. When pharmacologic agents increase mineral content or suppress turnover, they can shift the scan in a favorable direction without necessarily restoring the dynamic biology that makes bone resilient.
To understand this properly, it helps to separate three concepts: bone mineral density (BMD), bone turnover, and bone quality. DEXA quantifies areal BMD, which reflects mineral content projected over an area. It does not measure microcracks, collagen cross-link integrity, cortical thickness distribution, trabecular connectivity, or the mechanical properties of the matrix. Reviews in bone biomechanics emphasize that bone strength is determined by both density and quality, including microarchitecture and matrix composition. (NIH PMC: Bone Quality and Fracture Risk; NIH PMC: Material and Structural Determinants of Bone Strength)
When a medication alters remodeling dynamics in a way that increases mineral packing but impairs the bone’s ability to renew itself, the result can be bone that is denser on paper yet less capable of absorbing force.
1. Anti-Resorptives: Suppressing Turnover Can Increase Density While Reducing Remodeling
Drugs such as bisphosphonates and denosumab are classified as anti-resorptives. They work primarily by suppressing osteoclast activity, slowing the breakdown side of bone remodeling. This typically leads to increases in BMD on DEXA scans and reductions in certain fracture types in clinical trials, particularly vertebral fractures.
The mechanism is not true rebuilding of bone architecture in the sense of restoring youthful remodeling dynamics. Instead, it suppresses bone turnover. Remodeling is not optional maintenance; it is how bone repairs microdamage. When turnover is chronically suppressed, microcracks can accumulate. Over time, this can alter the material properties of bone, increasing brittleness despite higher mineral density.
Long-term bisphosphonate use has been associated with atypical femoral fractures, a phenomenon thought to be linked to severely suppressed bone turnover and altered material properties. Reviews in The New England Journal of Medicine and other major journals have examined this complication in the context of prolonged anti-resorptive therapy. (NEJM: Atypical Femoral Fractures and Bisphosphonates; PubMed indexed reviews on suppressed bone turnover and microdamage accumulation)
This does not mean these drugs have no place. It means that increasing mineral density is not synonymous with restoring bone vitality.
2. Over-Mineralization Can Make Bone More Brittle
Bone needs the correct balance between mineral and matrix. Excessive mineralization relative to collagen can make bone stiffer but less tough. Toughness refers to the ability of bone to absorb energy before fracturing. If bone becomes overly mineralized without adequate collagen renewal and microarchitectural repair, it can behave more like ceramic than living tissue.
Research into bone material properties has shown that alterations in collagen cross-linking and mineral crystal characteristics influence fracture resistance independent of BMD. (NIH PMC: Collagen Cross-Links and Bone Mechanical Properties; Journal of Bone and Mineral Research material property studies)
Anti-resorptives reduce remodeling cycles. Fewer remodeling cycles mean fewer opportunities to replace aged collagen and correct microdamage. The DEXA scan may register higher mineral content because old bone remains in place longer. What the scan does not reveal is whether that bone has become structurally fatigued.
3. Anabolic Agents: More Complex, But Still Not a Full Reset
Anabolic drugs such as teriparatide and abaloparatide stimulate bone formation by acting on parathyroid hormone pathways. These agents can increase BMD and improve certain microarchitectural parameters more robustly than anti-resorptives. However, their use is time-limited, and gains are often followed by anti-resorptive therapy to maintain density.
Even here, the rebuilding process is pharmacologically driven and does not automatically correct upstream drivers such as chronic inflammation, endocrine imbalance, protein insufficiency, glucocorticoid exposure, or inadequate mechanical loading. If those drivers remain unaddressed, the biology that led to fragility in the first place is still active.
Clinical trials of teriparatide demonstrate improvements in BMD and reductions in vertebral fractures, yet these outcomes occur within a framework of targeted pharmacologic stimulation, not comprehensive restoration of bone physiology. (PubMed: Teriparatide and Fracture Reduction Trials)
Medication-induced density increases do not replace the need for collagen integrity, muscle strength, and hormonal balance.
4. The DEXA Illusion: Density Is Not Architecture
DEXA scanning is a two-dimensional projection. It cannot distinguish between healthy trabecular connectivity and mineral filling of previously porous regions. It cannot measure cortical porosity directly in the way high-resolution peripheral quantitative CT can. It cannot evaluate collagen cross-link patterns or microdamage burden.
Studies examining the relationship between BMD and fracture risk show that many fractures occur in individuals who do not meet densitometric criteria for osteoporosis. This underscores the limits of relying solely on BMD as a proxy for strength. (NIH PMC: Fractures in Patients Without Osteoporosis by BMD Criteria)
A rise in BMD from −2.7 to −2.1 may look like success on paper. It does not confirm that bone toughness, structural anisotropy, and repair capacity have normalized.
5. Suppressed Turnover and Atypical Fracture Patterns
One of the clearest clinical signals that density alone is insufficient comes from atypical femoral fractures seen in patients on long-term bisphosphonate therapy. These fractures occur with minimal trauma and exhibit distinctive radiographic patterns. Research suggests that prolonged suppression of bone turnover contributes to accumulation of microdamage and altered material properties. (PubMed: Bisphosphonate-Associated Atypical Femoral Fractures)
The paradox is sobering: bone can test denser while becoming less capable of distributing mechanical stress.
Again, this is not an argument for abandoning therapy in high-risk individuals. It is an argument for recognizing that density improvement is not the same as biologic restoration.
6. Bone Is a Living Tissue, Not a Storage Depot
True rebuilding of bone requires coordinated remodeling. Osteoclasts remove old or damaged bone. Osteoblasts lay down new collagen matrix. That matrix mineralizes in a regulated fashion. Hormones, cytokines, mechanical strain, and nutrient availability all modulate this cycle.
When a drug freezes one side of the equation for extended periods, it changes the dynamics of renewal. The skeleton may become quieter on lab markers and denser on scans, yet less adaptive. Living tissue that cannot remodel properly becomes aged tissue.
The long-term goal should not be to silence bone turnover but to normalize it.
7. What Actually Rebuilds Resilient Bone
Rebuilding bone in a way that improves both density and quality requires:
- Progressive mechanical loading that stimulates osteogenesis through strain signaling
- Adequate protein intake to support collagen matrix formation
- Sufficient vitamin C and micronutrients required for collagen synthesis
- Optimization of estrogen, thyroid, cortisol, and metabolic health
- Strategic, individualized use of pharmacologic therapy when fracture risk justifies it
High-intensity resistance training trials demonstrate improvements in parameters related to bone strength and function, addressing not just density but also neuromuscular resilience. (PubMed: LIFTMOR Trial)
Protein intake is consistently associated with improved BMD and lower fracture risk in older adults, reinforcing the importance of matrix support. (NIH PMC: Protein Intake and Bone Outcomes)
These strategies work upstream. They improve the instructions sent to bone, not merely the mineral deposited within it.
The Core Distinction
Prescription bone agents can increase mineral density. In appropriate high-risk patients, they reduce certain fracture risks, particularly vertebral fractures. That is clinically meaningful. However, they do not automatically restore collagen quality, normalize endocrine signaling, reverse chronic inflammation, or build muscle.
A higher DEXA score does not guarantee stronger bone in the mechanical sense. It confirms more mineral per projected area.
The real objective is resilient bone—bone that can bend microscopically, absorb force, and remodel efficiently. That requires living biology to function properly.
Density is a measurement. Resilience is a property. They overlap, but they are not identical.
If osteoporosis is framed solely as a mineral shortage, the intervention will chase mineral. If it is understood as a matrix-and-hormone disorder, the strategy becomes broader, more physiologic, and more aligned with how bone is actually built and maintained.
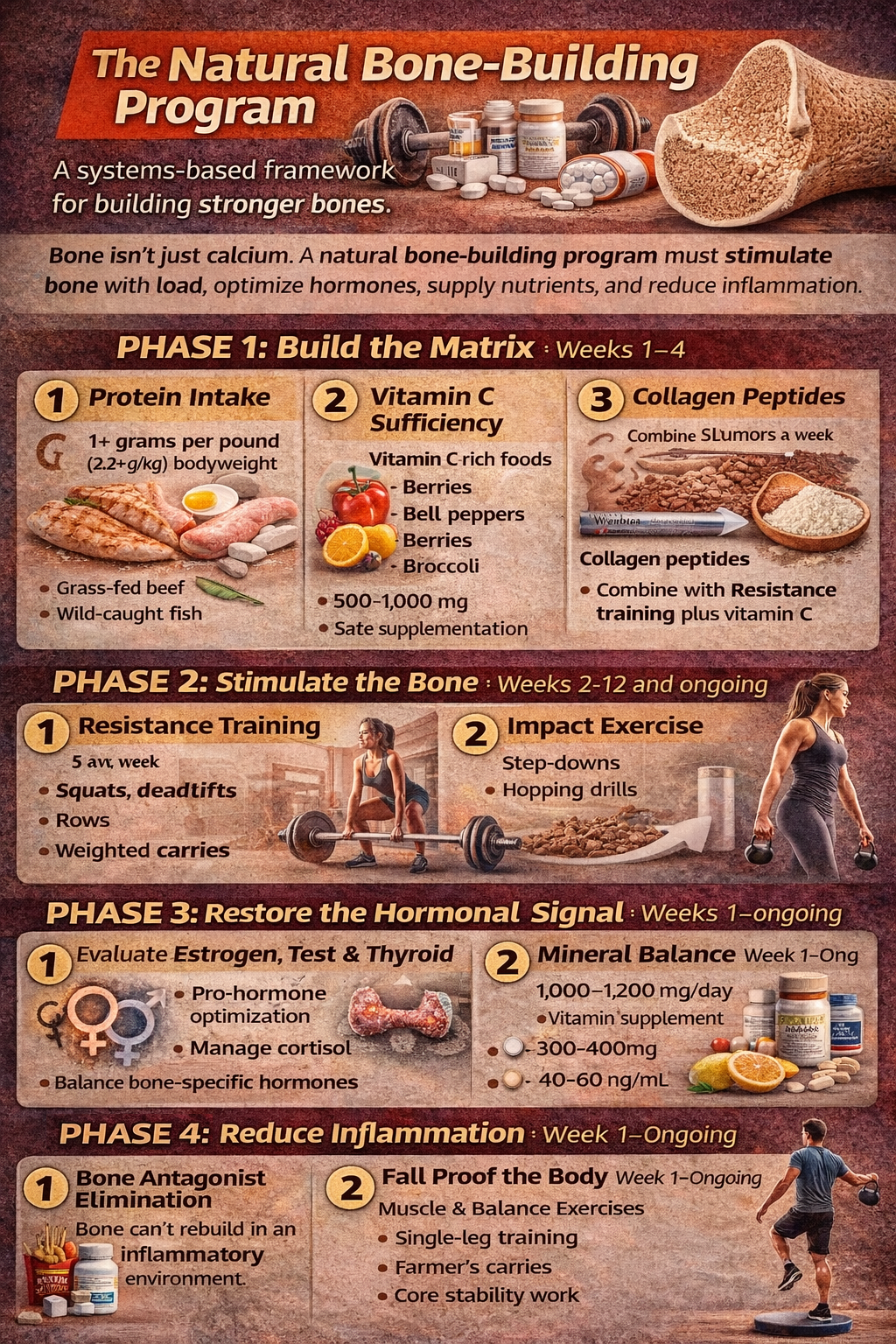
The Natural Bone-Building Program
Bone is not cement. It is living tissue that remodels in response to mechanical load, hormones, nutrient status, and inflammatory signals. A natural bone-building strategy must address all of those variables simultaneously. Increasing mineral intake without strengthening the collagen scaffold, restoring muscle mass, or correcting endocrine drivers is incomplete. What follows is a structured, physiology-centered program designed to improve bone density, bone quality, and fall resistance together.
This is educational material and not individualized medical advice. Anyone with prior fragility fractures, severe osteoporosis, complex endocrine disorders, kidney disease, or current prescription bone medications should work closely with a qualified clinician before implementing changes.
PHASE 1: BUILD THE MATRIX (Weeks 1–4)
1. Protein as Structural Medicine
Bone is roughly 30–40% organic matrix, largely type I collagen. Without sufficient amino acids, the scaffold cannot be rebuilt.
Target intake:
0.8–1.0 g protein per pound of ideal body weight for active adults (or 1.2–1.6 g/kg minimum in older adults).
Spread intake over 2–3 meals daily, aiming for 30–50 g high-quality protein per meal to stimulate muscle protein synthesis and collagen formation.
Best sources:
- Grass-fed beef
- Wild-caught fish
- Pasture-raised eggs
- Collagen-rich cuts (shank, oxtail, short ribs)
- Bone broth (adjunct, not sole source)
Pair protein intake with resistance training so amino acids are directed toward functional tissue rather than oxidation.
2. Vitamin C: The Collagen Catalyst
Vitamin C is required for hydroxylation of proline and lysine during collagen synthesis.
Food-first approach:
- Citrus
- Kiwi
- Bell peppers
- Berries
- Broccoli
Clinical range often used: 500–1,000 mg/day divided dosing when dietary intake is inconsistent.
Collagen without vitamin C is like bricks without mortar.
3. Strategic Collagen Support
Collagen peptides (10–15 g daily) may support bone matrix formation when combined with resistance training and sufficient protein intake. Best taken 30–60 minutes before training with vitamin C to enhance collagen synthesis signaling.
Collagen is not a substitute for protein; it complements it.
PHASE 2: STIMULATE THE BONE (Weeks 2–12 and ongoing)
Bone adapts to strain. Without progressive overload, there is no osteogenic signal.
4. Progressive Resistance Training (Non-Negotiable)
Minimum: 3 days per week.
Focus on multi-joint movements:
- Squats or sit-to-stands
- Deadlifts or hip hinges
- Overhead presses
- Rows
- Step-ups
- Loaded carries
Intensity matters. Research shows higher mechanical strain produces stronger osteogenic signaling than light “toning” exercise. Start supervised if fracture risk is high.
Principle:
Load the skeleton safely and progressively.
Walking is healthy but insufficient as a sole bone-building stimulus.
5. Impact (If Appropriate)
Low-level impact such as:
- Hopping drills
- Step-downs
- Brisk stair climbing
Avoid in individuals with high fracture risk unless supervised.
Impact stimulates trabecular adaptation in ways slow movement does not.
PHASE 3: RESTORE THE HORMONAL SIGNAL (Weeks 1–16)
Bone remodeling is hormonally regulated. If endocrine signals are misaligned, matrix and mineralization will suffer.
6. Estrogen & Testosterone Optimization
Postmenopausal estrogen decline accelerates bone resorption. In men, low testosterone correlates with decreased BMD.
Evaluate:
- Estradiol
- Free and total testosterone
- SHBG
- DHEA
Support through:
- Resistance training
- Body fat normalization
- Sleep restoration
- Stress reduction
Clinical hormone therapy decisions must be individualized.
7. Thyroid Balance
Excess thyroid hormone increases turnover and can weaken bone.
Evaluate:
- TSH
- Free T3
- Free T4
- Reverse T3 if indicated
Avoid over-replacement if on thyroid medication. Bone is highly sensitive to thyroid signaling.
8. Cortisol Control
Chronic stress and glucocorticoids accelerate bone breakdown.
Strategies:
- 7–9 hours sleep
- Strength training (not chronic endurance overload)
- Breathwork and parasympathetic activation
- Eliminate unnecessary steroid exposure
Bone cannot rebuild in a chronic catabolic state.
PHASE 4: MINERAL BALANCE (Weeks 1–Ongoing)
9. Calcium — Adequate, Not Excessive
Target total intake: 1,000–1,200 mg/day from diet first.
Sources:
- Sardines with bones
- Leafy greens
- Dairy (if tolerated)
- Mineral-rich water
Supplement only if dietary intake is insufficient and risk profile supports it.
Calcium is a building material, not a foreman.
10. Magnesium: The Overlooked Cofactor
Magnesium supports vitamin D metabolism and bone matrix quality.
Target intake: 300–400 mg/day (diet + supplement).
Sources:
- Pumpkin seeds
- Dark leafy greens
- Almonds
- Magnesium glycinate or malate supplementation if needed
Bone metabolism is mineral-cofactor dependent.
11. Vitamin D — Hormonal, Not Just Nutritional
Vitamin D regulates calcium absorption and osteoblast function.
Target blood 25(OH)D: commonly 40–60 ng/mL (individualized).
Sunlight is ideal when available. Supplementation often required depending on geography and season.
12. Vitamin K2 (Adjunct)
K2 helps regulate osteocalcin activation and calcium distribution.
Common supplemental range: 90–180 mcg MK-7 daily.
Acts as a traffic director for calcium, not a builder.
PHASE 5: REDUCE INFLAMMATION & TOXIC BURDEN
Chronic inflammation accelerates bone resorption.
13. Eliminate Bone Antagonists
Reduce:
- Refined sugar
- Ultra-processed seed oils
- Excess alcohol
- Smoking
Control:
- Insulin resistance
- Chronic inflammatory conditions
Hyperglycemia increases collagen glycation, making bone more brittle.
PHASE 6: FALL PROOF THE BODY
Many fractures occur because of falls, not spontaneous collapse.
14. Muscle & Balance
- Single-leg training
- Farmer’s carries
- Core stability work
- Tai chi or balance drills
WEEKLY STRUCTURE EXAMPLE
Monday: Lower body strength + collagen + vitamin C
Tuesday: Active recovery + mobility
Wednesday: Upper body strength + balance drills
Thursday: Brisk walking or stairs
Friday: Full-body strength session
Saturday: Optional impact work (if appropriate)
Sunday: Rest + recovery focus
WHAT THIS PROGRAM DOES DIFFERENTLY
• Builds collagen, not just mineral
• Stimulates bone with mechanical load
• Optimizes endocrine signaling
• Supports mineral metabolism intelligently
• Reduces inflammation that accelerates breakdown
• Improves muscle and balance to prevent falls
This approach treats bone as living tissue rather than a static mineral bank.
EXPECTED TIMELINE
Weeks 4–6: Improved strength and stability
Weeks 8–12: Measurable increases in lean mass
Months 6–12: Potential improvement in bone density markers
12–24 months: Meaningful remodeling adaptation
Reference List for “Osteoporosis Isn’t a Calcium Deficiency — It’s a Collagen and Hormone Problem”
- Bone matrix composition and collagen dominance — PMC Article on Bone Matrix and Collagen in Bone Biology.
https://pmc.ncbi.nlm.nih.gov/articles/PMC2790195/ - Collagen peptides RCT in postmenopausal women — PubMed: Effects of Collagen Peptides on Bone Mineral Density and Bone Markers.
https://pubmed.ncbi.nlm.nih.gov/29337906/ - Collagen peptides in osteopenia and evolving evidence — PMC Review of Collagen Peptides and Bone Outcomes.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8441532/?utm_source=chatgpt.com - Vitamin C intake, BMD, and fracture risk (systematic review & meta-analysis) — Cambridge Journal: Vitamin C Intake in Relation to BMD and Fracture Risk.
https://www.cambridge.org/core/journals/british-journal-of-nutrition/article/vitamin-c-intake-in-relation-to-bone-mineral-density-and-risk-of-hip-fracture-and-osteoporosis-a-systematic-review-and-metaanalysis-of-observational-studies/E1229B088231CD96AE676352030F428B - Vitamin C and bone biology (emerging epigenetic and osteogenesis roles) — Journal of Bone and Mineral Research.
https://academic.oup.com/jbmr/advance-article/doi/10.1093/jbmr/zjaf174/8339886 - Protein intake and bone outcomes in older adults — PMC Article: Higher Protein Intake, BMD, and Lower Vertebral Fracture Risk.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8599066/ - High-intensity resistance and impact training in postmenopausal women (LIFTMOR trial) — PubMed: LIFTMOR Randomized Controlled Trial.
https://pubmed.ncbi.nlm.nih.gov/28975661/ - Estrogen plus progestin therapy and fracture outcomes (Women’s Health Initiative) — PubMed: WHI Hormone Therapy and Fracture Reduction.
https://pubmed.ncbi.nlm.nih.gov/14519707/ - Aromatase inhibitors and increased bone loss/fracture risk — PMC Article on Aromatase Inhibitor-Related Bone Loss.
https://pmc.ncbi.nlm.nih.gov/articles/PMC3846762/ - Subclinical thyroid dysfunction and fracture risk — JAMA Network Open: Thyroid Function and Fracture Risk.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2798206 - Glucocorticoid-induced osteoporosis mechanisms — The Lancet Article on Glucocorticoid Effects on Bone.
https://www.thelancet.com/journals/landia/article/PIIS2213-8587%2825%2900251-7/fulltext - Calcium supplementation efficacy and fracture prevention evidence — PMC Review of Calcium Supplementation Trials.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11821691/ - Magnesium intake and bone health results (meta-analysis) — PubMed Meta-Analysis: Magnesium and Bone Outcomes.
https://pubmed.ncbi.nlm.nih.gov/34666201/ - Vitamin K2 supplementation and bone outcomes (mixed clinical trials) — PubMed: Effects of Vitamin K2 (MK-7) on Bone
https://pubmed.ncbi.nlm.nih.gov/23525894/