The Best and Worst Sleeping Positions for Spinal Health
A Comprehensive Examination of Alignment, Biomechanics, and Long-Term Structural Outcomes
Sleep occupies approximately one third of the average adult life span. During those hours, the musculoskeletal system is not inactive; rather, it is undergoing cyclical loading, muscular relaxation, disc rehydration, and neurological recalibration. Because sleep represents a prolonged, sustained postural state, the mechanical stresses applied to the spine during this period can either support recovery or reinforce dysfunction. For individuals experiencing chronic neck stiffness, low back discomfort, radicular symptoms, or persistent morning tension, sleeping posture is often an overlooked yet influential contributor.
To understand why sleep position matters, it is necessary to revisit the fundamental architecture of the human spine. The spine is designed with three primary curves: cervical lordosis in the neck, thoracic kyphosis in the mid-back, and lumbar lordosis in the low back. These curves are not aesthetic features; they serve critical mechanical functions. They distribute compressive forces, protect neural structures, and optimize load-bearing efficiency. When these curves are maintained in a neutral orientation during sleep, passive structures such as ligaments and joint capsules are not excessively strained, and muscular tissues can downregulate tension appropriately. When these curves are flattened, exaggerated, or rotated for prolonged periods, mechanical stress accumulates.
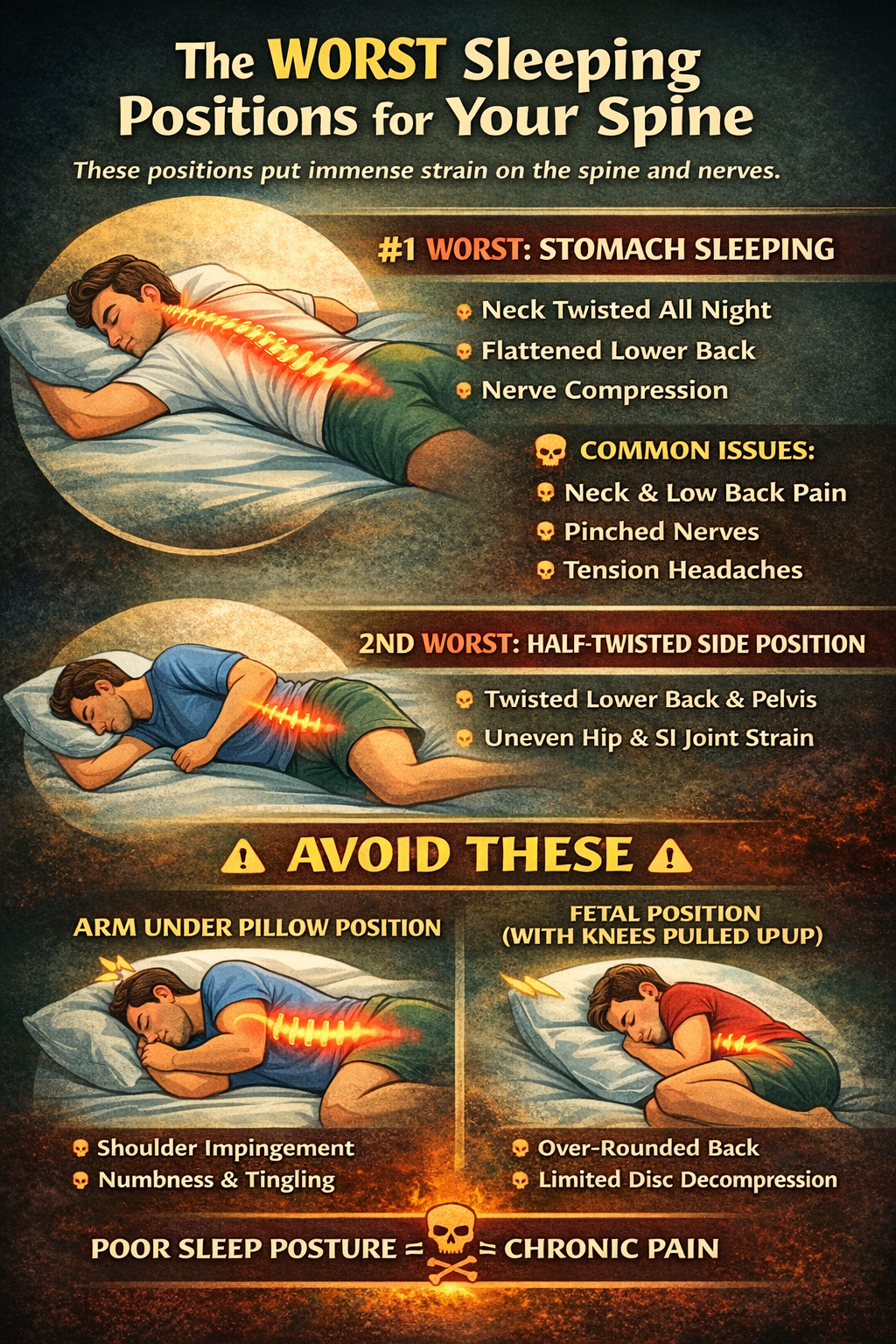
The Most Biomechanically Stressful Position: Prone (Stomach) Sleeping
Among common sleep positions, prone sleeping consistently imposes the greatest mechanical burden on the spine. The primary concern involves sustained cervical rotation. In order to breathe while lying face down, the head must be rotated sharply to one side. This rotational positioning is maintained for hours, placing asymmetric compression on the facet joints and creating torsional stress across cervical discs. Over time, this can contribute to chronic neck tightness, tension-type headaches, and localized joint irritation.
The lumbar spine is also affected in prone positioning. Depending on mattress firmness and abdominal support, the low back may either hyperextend or flatten inconsistently. Hyperextension increases posterior joint compression, while flattening reduces the natural lordotic curve and alters disc pressure distribution. Both scenarios compromise ideal biomechanics. In addition, the thoracic spine often compensates for cervical rotation, leading to subtle mid-back torsion. This cumulative rotational stress can influence shoulder mechanics and scapular positioning, potentially contributing to upper quarter dysfunction.
While some individuals report temporary comfort in prone sleeping, particularly those with certain disc presentations, the long-term mechanical implications generally outweigh short-term relief. For most adults, stomach sleeping should be minimized or gradually transitioned away from.
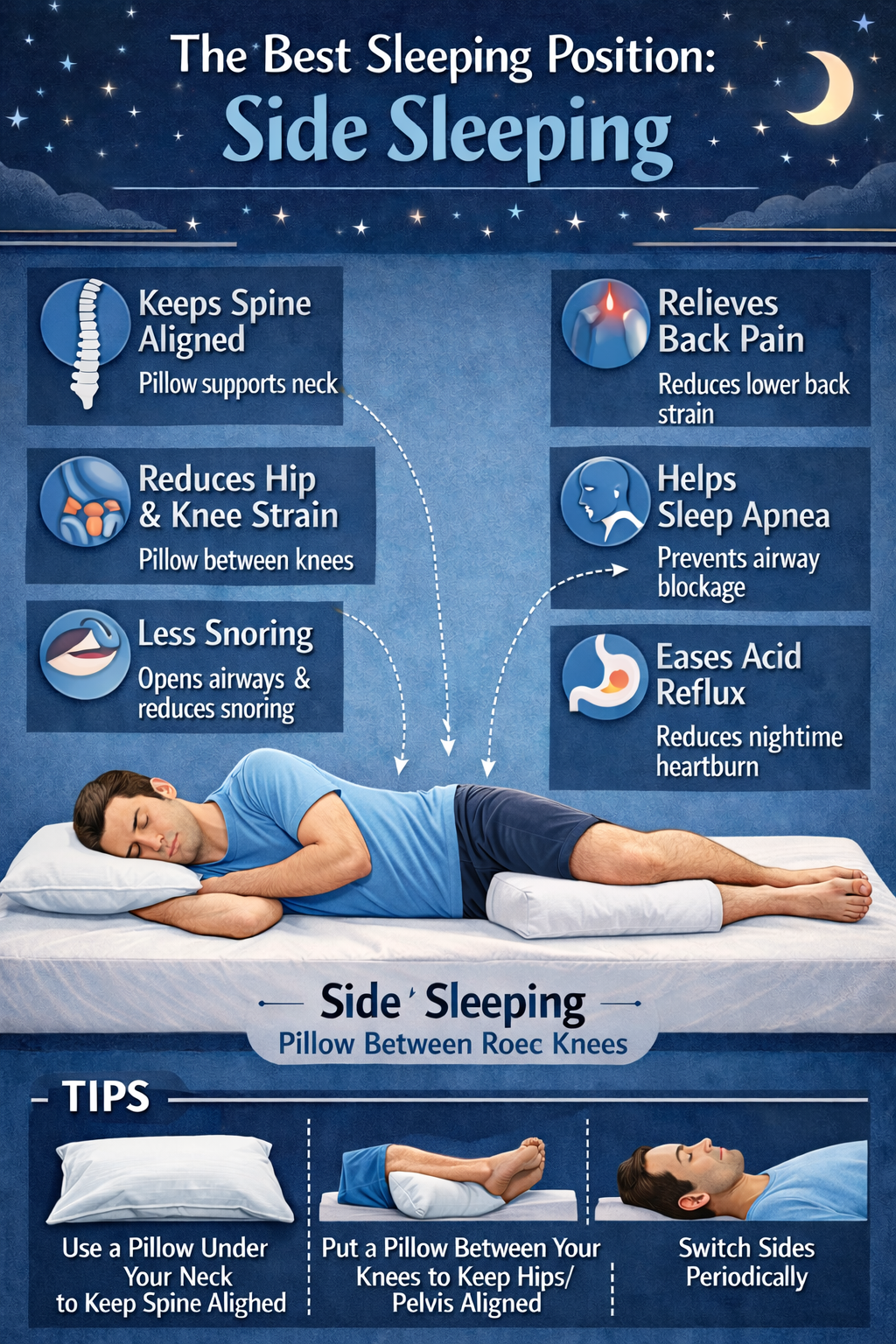
Side Sleeping: Beneficial When Structured Correctly
Side sleeping is widely regarded as a favorable spinal position, yet its benefits depend entirely on proper support. When executed with attention to alignment, lateral sleeping can maintain relatively neutral spinal curves while minimizing rotational strain.
The first consideration is cervical alignment. The pillow must adequately fill the space between the lateral shoulder and the head. If the pillow is too thin, the head drops laterally toward the mattress, placing the cervical spine into side bending. If too thick, the head tilts upward, creating the opposite distortion. Either deviation increases muscular guarding and joint stress. A well-fitted pillow maintains the head in line with the thoracic spine, preserving neutral alignment.
Pelvic positioning is equally important. Without support between the knees, the top leg tends to fall forward, pulling the pelvis into rotation and transmitting torsional forces into the lumbar spine. Placing a firm pillow between the knees helps maintain pelvic neutrality and reduces strain on the sacroiliac joints. For individuals with recurrent low back or SI joint discomfort, this adjustment can be significant.
When cervical and pelvic alignment are maintained, side sleeping allows for more balanced disc loading and reduces compressive stress compared to prone positioning. Additionally, side sleeping may support improved airway patency in individuals prone to snoring or mild airway collapse, indirectly reducing muscular tension associated with fragmented sleep.
The Common Side-Sleeping Error: Rotational Drift
It is important to distinguish structured side sleeping from the “half-twist” posture frequently observed. In this variation, one leg remains extended while the other crosses forward, subtly rotating the pelvis. The torso may also roll partially toward the mattress, creating combined flexion and rotation in the lumbar region. Although this posture may feel comfortable initially, prolonged rotational stress can contribute to asymmetrical muscle tone and perceived pelvic imbalance. Corrective support, including a knee pillow and occasionally a small waist support roll, can mitigate this tendency.
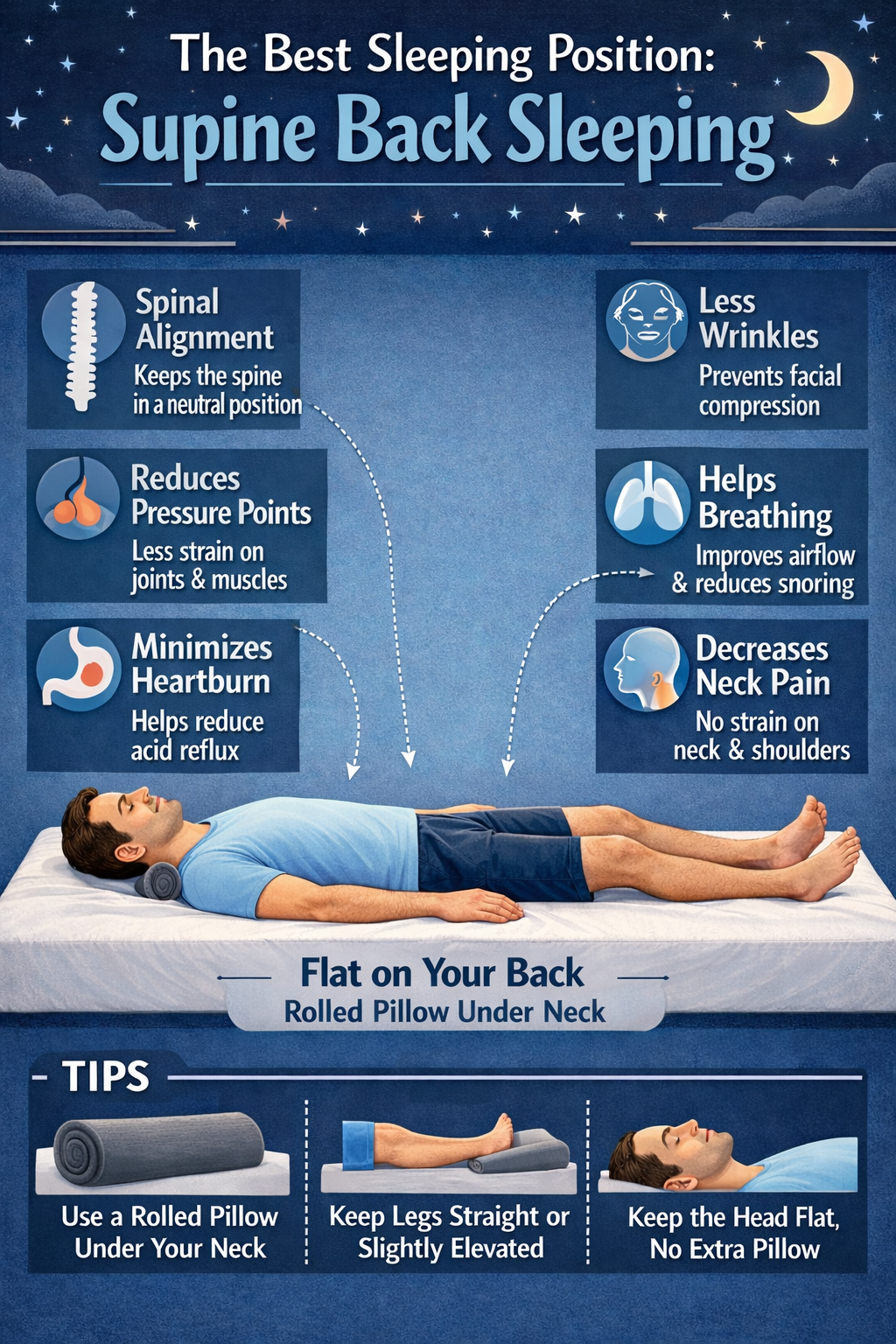
Supine (Back) Sleeping: Symmetry with Conditions
Sleeping on the back provides symmetrical weight distribution and eliminates rotational stress. From a structural standpoint, this position can be highly supportive, particularly for individuals with certain disc pathologies or those seeking uniform spinal loading.
However, supine positioning introduces two potential concerns.
– First, without support beneath the knees, the lumbar spine may remain in relative extension, increasing posterior joint compression. Elevating the knees slightly with a pillow reduces lumbar stress by encouraging gentle hip flexion.
– Second, pillows. Any and all pillows when sleeping on your back create forward head posture. Do not use a pillow when sleeping on your back, instead use a 3″ spinal mold for your neck. This will ensure proper cervical curve as your skull must remain touching the mattress when sleeping on your back.
Excessively thick pillows push the head forward into cervical flexion. Cervical contour pillows designed to maintain neutral curvature may be beneficial when properly fitted.
It should also be noted that back sleeping can exacerbate snoring or obstructive sleep apnea in susceptible individuals. In such cases, airway considerations may supersede purely structural preferences, and lateral positioning may be more appropriate.
Mattress and Surface Considerations
Sleeping position cannot be evaluated independently of mattress characteristics. A mattress that is too soft allows excessive spinal sinking, promoting flexion and curve collapse. A mattress that is too firm may create pressure points and reduce the ability of the spine to maintain natural curvature. The optimal surface permits slight contouring while preserving structural support. Individual body weight, distribution, and existing spinal conditions influence ideal firmness levels.
Clinical Implications of Prolonged Postural Stress
Prolonged nocturnal misalignment can contribute to repetitive low-grade strain on passive spinal structures. Ligamentous creep, asymmetrical disc loading, and chronic muscle guarding may develop gradually. Patients frequently report that morning discomfort improves as the day progresses, suggesting that sleep posture is contributing to cumulative stress rather than acute injury. While sleep position alone rarely causes severe pathology, it can perpetuate existing dysfunction.
Practical Recommendations
For individuals seeking to optimize spinal health during sleep, the following principles are recommended:
- Avoid sustained prone sleeping whenever possible.
- If side sleeping, use a pillow of appropriate height and place support between the knees.
- If back sleeping, support the knees and ensure neutral cervical positioning.
- Periodically reassess mattress integrity, particularly if it is more than seven to ten years old.
- Monitor morning symptoms as feedback regarding positional adequacy.
Conclusion
Sleeping posture represents a sustained mechanical input applied nightly over decades. The spine, as the structural housing for the central nervous system, responds predictably to prolonged stress. Positions that preserve natural curvature and minimize rotational strain support restorative processes that occur during sleep, including disc hydration and muscular relaxation. Positions that distort alignment may reinforce dysfunction and contribute to persistent discomfort.
Optimal sleep positioning does not require complex intervention; rather, it requires attention to neutrality, support, and mechanical consistency. Over time, these adjustments can contribute meaningfully to long-term spinal resilience and overall structural integrity.