The Common Thread We’ve Been Missing
Modern medicine has become extraordinarily skilled at categorizing disease.
Cardiology treats the heart.
Endocrinology treats blood sugar.
Neurology treats memory loss.
Oncology treats abnormal cell growth.
But what if these conditions are not as separate as we’ve been taught?
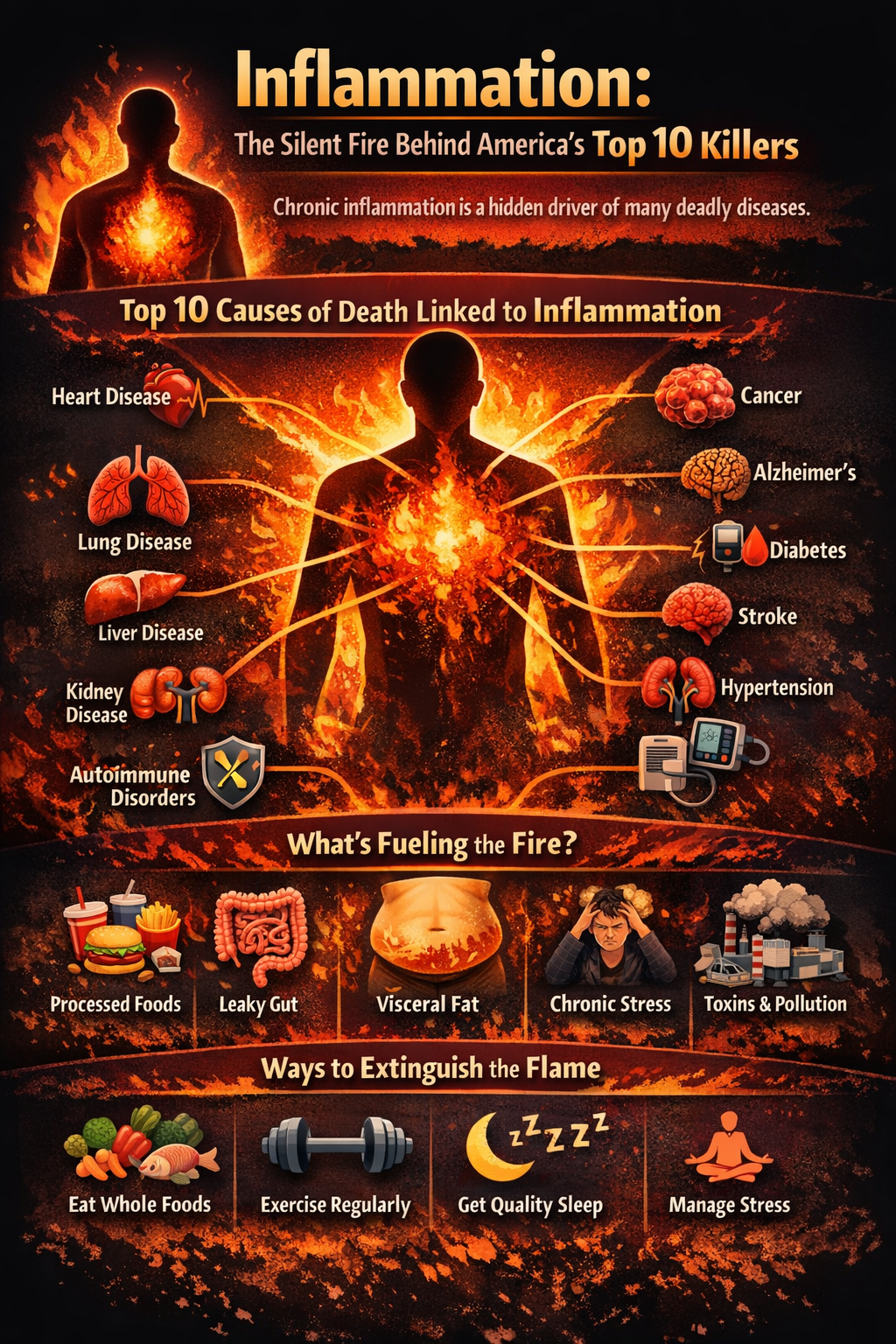
What if the leading causes of death in the United States share a deeper biological thread — one that begins long before symptoms appear?
That thread is chronic inflammation.
Not the swelling you feel after an injury. Not the fever that accompanies infection. But a persistent, low-grade immune activation that quietly alters tissues over years or decades.
When we examine heart disease, diabetes, Alzheimer’s, cancer, stroke, kidney disease, liver disease, and autoimmune disorders at the cellular level, a recurring pattern emerges: sustained inflammatory signaling that disrupts normal physiology.
Inflammation: Protective Mechanism Turned Pathological
Inflammation is not inherently harmful. It is essential to survival.
When tissue is injured or invaded by pathogens, immune cells release signaling molecules — cytokines, chemokines, prostaglandins — that coordinate repair. Blood vessels dilate, immune cells migrate, debris is cleared, and healing occurs.
This is acute inflammation. It is time-limited and self-resolving.
Chronic inflammation is different.
It represents a failure to return to baseline. Instead of resolving, immune signaling persists. Cytokines remain elevated. Oxidative stress increases. Cellular repair mechanisms become strained.
The result is not dramatic swelling. It is gradual dysfunction.
Arteries stiffen. Insulin receptors lose sensitivity. Neurons become vulnerable. Mitochondria produce less energy. Cellular communication becomes distorted.
Inflammation shifts from protector to disruptor.
Heart Disease: An Inflammatory Process, Not Just a Lipid Disorder
For decades, cardiovascular disease was framed primarily as a cholesterol storage problem. But arterial plaque is not simply a passive accumulation of fat.
It is an active immune response.
Low-density lipoprotein (LDL) particles can become oxidized within the arterial wall. Oxidized LDL triggers immune recognition. Macrophages engulf these particles, forming foam cells. Inflammatory cytokines are released. Smooth muscle cells proliferate. The arterial lining thickens.
This process — atherosclerosis — is fundamentally inflammatory.
C-reactive protein (CRP), an inflammatory marker, often predicts cardiovascular risk independently of cholesterol levels. Individuals with modest LDL but high inflammatory markers can be at greater risk than those with higher LDL but low inflammation.
Plaque instability, which leads to rupture and clot formation, is closely tied to inflammatory activity within the vessel wall.
The heart attack is often the endpoint of decades of silent immune activation.
Type 2 Diabetes: A Metabolic and Immune Disorder
Type 2 diabetes is typically defined by elevated blood glucose. Yet hyperglycemia is the outcome, not the origin.
Chronic inflammation interferes with insulin signaling. Cytokines such as TNF-alpha impair insulin receptor function and reduce glucose uptake into cells.
Visceral adipose tissue — fat surrounding abdominal organs — is metabolically active. It secretes inflammatory mediators known as adipokines. As visceral fat increases, inflammatory signaling intensifies.
This inflammatory environment promotes insulin resistance. The pancreas compensates by producing more insulin. Over time, beta cells fatigue.
Elevated blood sugar then generates additional oxidative stress, perpetuating the cycle.
Diabetes is not solely about sugar consumption. It is deeply intertwined with immune dysregulation.
Alzheimer’s Disease: Neuroinflammation and Cognitive Decline
Neurodegenerative disease is increasingly understood through the lens of inflammation.
Microglia, the immune cells of the central nervous system, become chronically activated in Alzheimer’s disease. They release inflammatory mediators that damage neurons and impair synaptic function.
Systemic inflammation can influence the brain through blood-brain barrier permeability and circulating cytokines. Chronic immune activation may accelerate amyloid deposition and tau pathology.
Cognitive decline is not simply a function of aging. It reflects a shift in the inflammatory environment of the brain.
The brain, like every organ, responds to systemic physiology.
Cancer: When Immune Signaling Supports Tumor Growth
The relationship between inflammation and cancer is complex.
Chronic inflammatory states increase oxidative stress and DNA damage. They promote angiogenesis — the formation of new blood vessels that tumors require. They alter immune surveillance, sometimes allowing abnormal cells to evade detection.
Conditions characterized by persistent inflammation — such as chronic hepatitis or inflammatory bowel disease — are associated with increased cancer risk in affected tissues.
While inflammation is part of the body’s defense system, sustained inflammatory signaling can create a microenvironment that supports tumor progression.
The same immune mechanisms designed to protect can, under chronic stimulation, facilitate disease.
Chronic Respiratory Disease, Kidney Disease, and Liver Disease
Inflammation also underlies chronic lower respiratory disease, including chronic obstructive pulmonary disease (COPD). Persistent immune activation damages airway structures and impairs gas exchange.
In chronic kidney disease, inflammatory mediators contribute to fibrosis and declining filtration capacity.
Non-alcoholic fatty liver disease is strongly linked to metabolic inflammation, insulin resistance, and oxidative stress.
Across organ systems, the pattern remains consistent: immune activation that fails to resolve leads to progressive structural and functional damage.
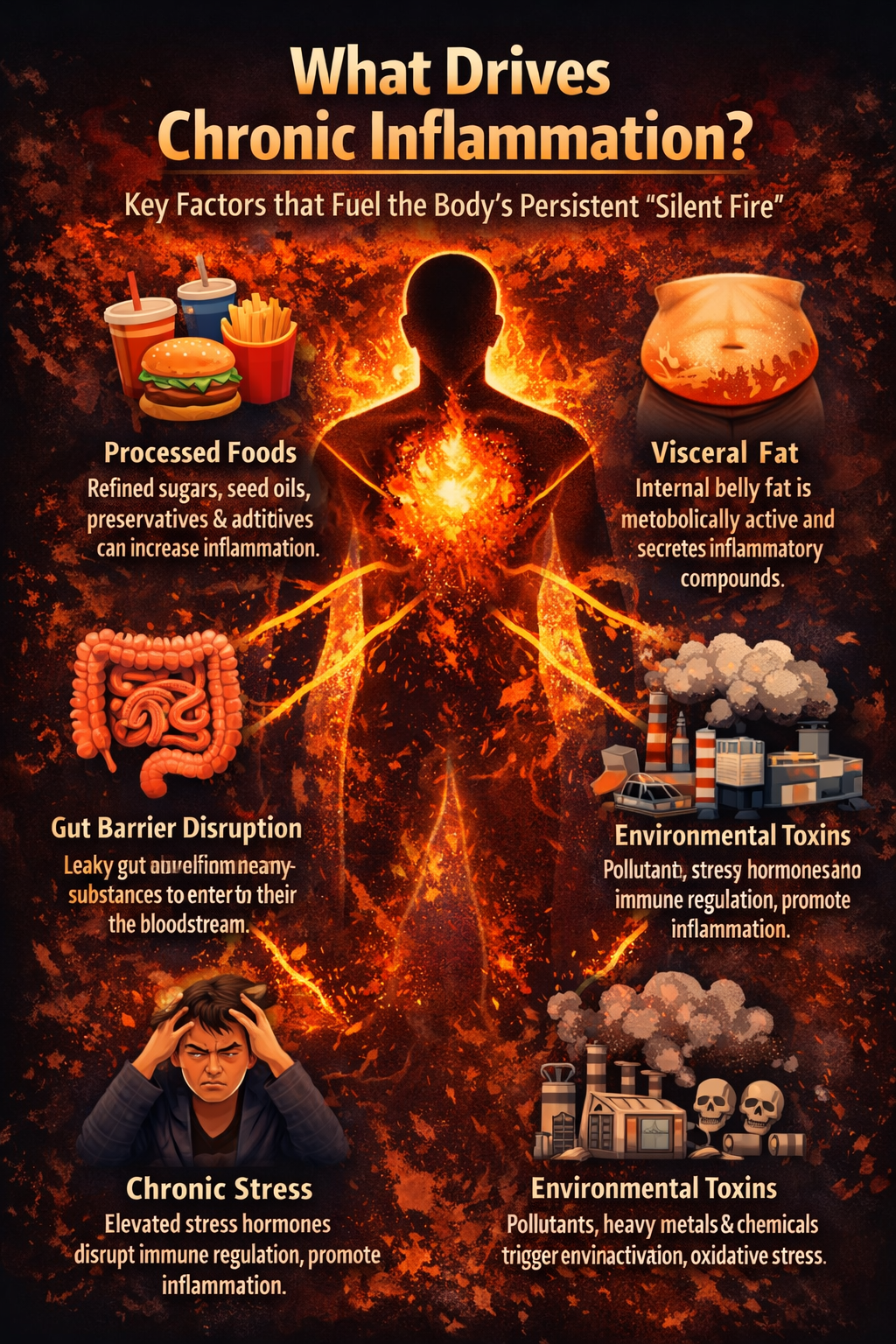
What Sustains Chronic Inflammation?
Inflammation does not persist without cause. It is continually stimulated by environmental and metabolic inputs.
1. Metabolic Overload and Blood Sugar Instability
Frequent spikes in blood glucose increase oxidative stress and promote inflammatory signaling pathways such as NF-kB activation.
Advanced glycation end products (AGEs), formed when glucose binds proteins, further stimulate immune responses. Metabolic instability feeds inflammatory cascades.
2. Visceral Adiposity
Excess abdominal fat functions as an endocrine organ. It secretes inflammatory cytokines and contributes to insulin resistance.
As adipose tissue expands, immune cell infiltration increases, amplifying inflammatory output. The distribution of fat matters as much as total body weight.
3. Gut Barrier Dysfunction
The intestinal lining serves as a selective barrier. When permeability increases, microbial fragments such as lipopolysaccharides (LPS) can enter circulation.
Even small quantities of LPS can provoke systemic immune activation. The gut is a major interface between the external environment and the immune system. Barrier integrity is central to inflammatory balance.
4. Chronic Psychological Stress
Stress activates the hypothalamic-pituitary-adrenal (HPA) axis and sympathetic nervous system. Over time, dysregulated cortisol rhythms and persistent adrenergic signaling alter immune modulation.
Chronic stress can shift the immune system toward a pro-inflammatory state. Emotional and physiological stress are not separate domains.
5. Sleep Disruption
Inadequate sleep increases inflammatory markers, impairs glucose metabolism, and alters immune cell behavior.
Sleep is a biological repair state. Without sufficient restorative sleep, inflammatory tone rises.
6. Environmental Exposures
Air pollution, heavy metals, endocrine-disrupting chemicals, and other environmental toxins can trigger oxidative stress and immune activation.
The body possesses detoxification systems, but chronic exposure can overwhelm these pathways.
The Inflammatory Network
Chronic inflammation is not linear. It is networked.
Metabolic dysfunction increases inflammatory signaling. Inflammation worsens insulin resistance. Insulin resistance increases visceral fat. Visceral fat amplifies cytokine production.
Gut permeability increases systemic inflammation. Inflammation alters gut microbiota. Dysbiosis further impairs barrier function.
Stress disrupts sleep. Poor sleep worsens glucose control. Glucose instability feeds inflammation. The system is interconnected. Effective intervention must acknowledge that interdependence.

A Systems Approach to Reducing Inflammation
Suppressing inflammation without addressing its drivers is unlikely to produce lasting change.
A more effective strategy involves modifying the inputs that sustain immune activation.
Stabilize Glucose Regulation
Reducing refined carbohydrates and improving metabolic flexibility decreases oxidative stress and inflammatory signaling.
Balanced macronutrient intake and adequate fiber support glycemic stability.
Improve Body Composition
Resistance training and regular movement enhance insulin sensitivity and reduce inflammatory adipokines associated with visceral fat.
Muscle tissue improves metabolic resilience.
Restore Gut Integrity
Dietary diversity, adequate fiber, and minimizing dietary irritants support microbiome health and barrier function.
Gut integrity reduces systemic immune activation.
Prioritize Sleep Architecture
Consistent sleep timing, reduced evening light exposure, and minimizing sleep disruption restore circadian rhythms and immune balance.
Regulate Stress Physiology
Breathing exercises, contemplative practices, time in nature, and meaningful social connection modulate autonomic tone and reduce inflammatory signaling.
Reduce Toxic Burden
Improving air quality, water filtration, and minimizing unnecessary chemical exposure can decrease chronic immune stimulation.
The Larger Implication
Inflammation is not a diagnosis. It is a biological state.
When chronic inflammation persists, it increases the probability of disease across multiple organ systems. When inflammatory load decreases, metabolic, vascular, and neurological function often improve in parallel.
The leading causes of death in America may appear distinct on paper. At the cellular level, they share a common disturbance in immune regulation.
The question is not whether inflammation is present. The question is whether we are addressing its drivers early — before irreversible damage occurs. Chronic disease rarely begins abruptly. It develops gradually within an inflammatory environment.
And that environment is modifiable. The body is not passive in the face of change. It responds dynamically to shifts in nutrition, sleep, stress, movement, and exposure.
When the inputs change, the biology follows. Inflammation does not have to be permanent. But it does have to be understood.