Why Chronic Viral Infections Are Rarely Explored in Long-Term Disease
Modern medicine excels at identifying and managing acute infections. A patient presents with fever, rash, swollen glands, or respiratory distress; diagnostic testing is performed; treatment is administered; the infection resolves. The episode is considered closed. This acute-care model works well for immediate threats but becomes far less effective when symptoms persist beyond the expected timeline.
Chronic illness does not fit neatly into the acute infection paradigm. When patients develop prolonged fatigue, unexplained anemia, chronic joint pain, cognitive changes, or inflammatory symptoms, the diagnostic approach often shifts toward autoimmune classification, psychiatric attribution, or symptomatic management. Rarely does the investigation continue into the possibility of persistent viral activity—especially if the original infection was mild or occurred years earlier.
There are structural reasons for this. Chronic viral persistence is difficult to measure. Antibody levels may normalize. Viral DNA may be intermittently detectable. Standard panels do not routinely screen for viral reservoirs in tissues. As a result, persistent viral triggers are often underappreciated in chronic inflammatory conditions.
One virus that illustrates this gap particularly well is Parvovirus B19.
What Is Parvovirus B19?

Parvovirus B19 is a small, non-enveloped, single-stranded DNA virus belonging to the Parvoviridae family. It infects humans exclusively and has a strong tropism—meaning tissue preference—for erythroid progenitor cells in the bone marrow. These are the cells responsible for producing red blood cells.
The virus binds to the P antigen (globoside) receptor, which is expressed on erythroid precursors and certain endothelial and myocardial cells. This receptor distribution explains many of the clinical features seen in both acute and chronic infection.
Parvovirus B19 is best known as the cause of erythema infectiosum, commonly called “fifth disease,” a childhood illness characterized by a bright red facial rash. Because the pediatric presentation is usually mild and self-limited, the virus is often regarded as trivial. However, its biological behavior in adults, pregnant women, and individuals with immune dysregulation can be far more complex.
Epidemiology and Transmission
Parvovirus B19 is widespread globally. Seroprevalence studies show that approximately 50–60% of adults have detectable IgG antibodies, indicating prior exposure. By older adulthood, that percentage may exceed 70%.
Transmission occurs primarily through:
- Respiratory droplets
- Close household contact
- Blood transfusion (rare but documented)
- Vertical transmission from mother to fetus
Infections are more common in late winter and spring, often in school or daycare settings. Adults typically acquire infection from children.
Importantly, individuals are most contagious during the viremic phase—before the rash appears. Once the rash develops, viral replication is usually declining.
Pathophysiology: What the Virus Actually Does
After inhalation, Parvovirus B19 enters the bloodstream and travels to the bone marrow. There it infects erythroid progenitor cells and disrupts their maturation. The virus replicates inside these cells, leading to cell lysis and temporary suppression of red blood cell production.
In healthy individuals, this suppression is brief and clinically insignificant. However, in individuals with high red blood cell turnover (such as sickle cell disease or hereditary spherocytosis), even temporary suppression can precipitate an aplastic crisis.
Beyond bone marrow, viral DNA has been detected in:
- Synovial tissue
- Myocardial tissue
- Endothelial cells
- Peripheral nerves
The virus may not always actively replicate in these tissues but can persist in a low-level state, potentially contributing to chronic immune activation.
Acute Infection: Clinical Presentation
In Children
Acute infection in children typically presents with:
- Low-grade fever
- Mild malaise
- “Slapped cheek” facial rash
- Lacy, reticular rash on trunk and extremities
The rash appears after the viremic phase and usually resolves within 7–10 days. Most children recover completely.
In Adults
Adults often do not develop the classic rash. Instead, they present with:
- Symmetrical joint pain (hands, wrists, knees, ankles)
- Morning stiffness
- Fatigue
- Headache
- Low-grade fever
The joint symptoms may resemble early rheumatoid arthritis. In some adults, arthropathy persists for weeks to months.
Hematologic Effects
During acute infection, reticulocyte counts drop due to bone marrow suppression. This can lead to:
- Mild anemia
- Pallor
- Shortness of breath
In immunocompromised individuals, persistent infection can cause chronic pure red cell aplasia.
Chronic Parvovirus B19 Infection
The question that receives far less attention is what happens when the virus is not fully cleared.
Parvovirus B19 DNA has been identified in synovial biopsies of patients with chronic inflammatory arthritis, in myocardial tissue of patients with myocarditis, and in bone marrow of patients with chronic anemia. While the presence of viral DNA does not always equate to active infection, persistent viral fragments may sustain immune activation.
Chronic manifestations may include:
- Persistent or relapsing joint pain
- Chronic fatigue
- Anemia or fluctuating hemoglobin
- Myocardial inflammation
- Peripheral neuropathy
- Vasculitis
In some individuals, the immune response to viral antigens may contribute to autoimmune phenomena through molecular mimicry or chronic cytokine stimulation.
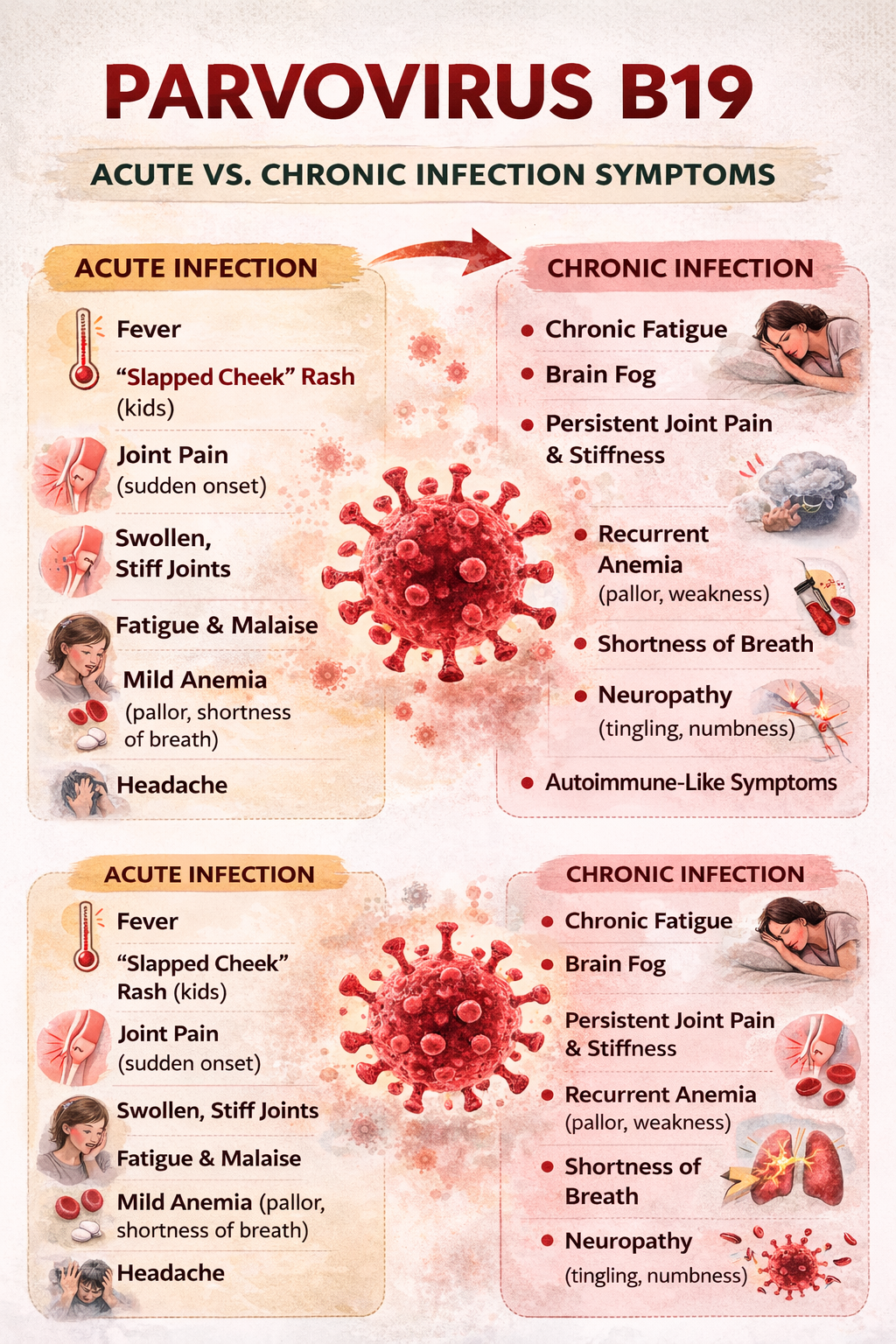
Acute vs Chronic Symptom Comparison
Acute Phase
- Fever
- Rash (common in children)
- Sudden joint pain
- Temporary anemia
- Headache
- Malaise
Chronic Phase
- Ongoing fatigue
- Persistent joint stiffness or swelling
- Exercise intolerance
- Cognitive slowing
- Recurrent anemia
- Neuropathic symptoms
Chronic symptoms may be subtle and fluctuate, making recognition difficult.
Diagnostic Testing
Accurate testing depends on timing and clinical suspicion.
1. Serology
- IgM antibodies indicate recent infection (usually detectable 7–10 days after exposure).
- IgG antibodies indicate past exposure and may persist lifelong.
Limitations:
- IgM may no longer be detectable in chronic cases.
- IgG does not confirm active infection.
2. PCR Testing
Polymerase chain reaction (PCR) detects viral DNA in blood or tissue.
Limitations:
- Blood PCR may be negative if virus is sequestered in tissue.
- Intermittent viremia may reduce detection sensitivity.
3. Bone Marrow Evaluation
In cases of unexplained chronic anemia, bone marrow biopsy may reveal viral inclusions and suppressed erythropoiesis.
No single test definitively confirms chronic active infection in all cases. Clinical context is essential.
Parvovirus B19 in Pregnancy
In pregnant women, acute infection can cross the placenta and infect the fetus. This may lead to:
- Fetal anemia
- Hydrops fetalis
- Miscarriage (in rare cases)
Pregnant women exposed to infected children should undergo evaluation if symptomatic.
Conventional Management
There is no specific antiviral medication approved for Parvovirus B19 in immunocompetent individuals. Treatment is generally supportive:
- NSAIDs for joint pain
- Monitoring of hemoglobin
- IVIG therapy in severe chronic anemia or immunocompromised patients
IVIG provides pooled antibodies that may neutralize circulating virus in severe cases.
Supporting Natural Viral Clearance and Immune Restoration
Chronic viral persistence is less about viral invincibility and more about immune dysregulation. Supporting viral resolution requires improving immune surveillance and reducing systemic inflammation.
1. Vitamin D Optimization
Vitamin D modulates innate and adaptive immunity. Adequate levels enhance antimicrobial peptide production and support regulatory T-cell balance.
Serum 25(OH)D levels between 40–60 ng/mL are often considered supportive for immune health, though individual needs vary.
2. Zinc Sufficiency
Zinc plays a critical role in antiviral defense and cellular immune signaling. Deficiency impairs T-cell function and increases susceptibility to infection.
Whole food sources include red meat and shellfish. Supplementation should be balanced with copper intake.
3. Glutathione and NAC
Chronic viral states often increase oxidative stress. N-acetylcysteine (NAC) supports glutathione production, which is essential for redox balance and immune cell function.
4. Anti-Inflammatory Nutrition
Diet profoundly influences immune regulation. A nutrient-dense diet emphasizing:
- High-quality proteins
- Omega-3 fatty acids
- Minimally processed carbohydrates
- Phytonutrient-rich vegetables
may reduce systemic inflammation and support immune efficiency.
Excess refined sugar and ultra-processed foods impair immune responsiveness.
5. Gut Integrity
The gut-associated lymphoid tissue (GALT) houses a large proportion of immune cells. Dysbiosis and increased intestinal permeability can contribute to chronic immune activation.
Strategies include:
- Removing inflammatory foods
- Supporting microbial diversity
- Ensuring adequate fiber intake (as tolerated)
- Considering targeted probiotics when indicated
6. Sleep and Circadian Regulation
Sleep deprivation suppresses natural killer cell activity and impairs antiviral defense. Consistent sleep timing and morning light exposure improve circadian alignment.
7. Botanical Antiviral Support
Some botanical compounds demonstrate antiviral properties in vitro:
- Olive leaf extract
- Andrographis
- Astragalus
- Elderberry
These should be used judiciously and under supervision, especially in individuals with autoimmune conditions.
8. Reducing Total Inflammatory Burden
Environmental toxins, chronic stress, and metabolic dysfunction strain immune capacity. Supporting detoxification pathways through:
- Hydration
- Regular bowel elimination
- Physical activity
- Sweating
may reduce overall inflammatory load.

In Conclusion
Parvovirus B19 is commonly dismissed as a mild childhood virus. Yet its biological characteristics—bone marrow tropism, endothelial interaction, and potential for persistence—suggest it may contribute to chronic inflammatory states in susceptible individuals.
It is not responsible for every unexplained illness. However, in patients with:
- Chronic unexplained anemia
- Persistent joint pain
- Post-viral fatigue
- Unresolved inflammatory syndromes
it deserves consideration.
Understanding Parvovirus B19 requires moving beyond the assumption that all viral infections are transient. Some leave footprints long after the acute phase resolves.
Identifying and addressing those footprints involves careful testing, clinical judgment, and comprehensive immune support.